Joana F. Pires, Sara Geraldes Paulino, Daniela Araújo, Francisco Miranda Antunes, Isabel Martinho
{"title":"肩胛骨急性血源性骨髓炎并发肩胛下脓肿:首例采用保守疗法的病例。","authors":"Joana F. Pires, Sara Geraldes Paulino, Daniela Araújo, Francisco Miranda Antunes, Isabel Martinho","doi":"10.1111/jpc.16695","DOIUrl":null,"url":null,"abstract":"<p>A previously healthy 3-year-old boy presented to the ED in May 2022 with pain and functional impairment of the left upper limb following a fall the previous day. The patient developed a fever while in the ED, with a peak temperature of 39°C noted during the initial physical examination. His physical examination revealed limited movement and pain in the left shoulder, with no skin lesions. Vital signs included a temperature of 39°C, heart rate of 115 bpm, respiratory rate of 20 breaths per minute, blood pressure of 98/53 mmHg and oxygen saturation of 100% on room air.</p><p>Initial diagnostic imaging, including plain radiography and ultrasound of the left shoulder, revealed no abnormalities. Laboratory results showed leukocytes 16 660/μL (neutrophils 15 000/μL), C-reactive protein 14.25 mg/L and sedimentation rate 54 mm/h. The patient was hospitalised with empirical intravenous cefuroxime (150 mg/kg/day) due to suspicion of osteoarticular infection. Blood cultures later grew methicillin-sensitive Staphylococcus aureus (MSSA), and treatment was adjusted to intravenous flucloxacillin (150 mg/kg/day).</p><p>MRI on the fourth day of hospitalisation revealed a large multiloculated abscess (6 cm × 4 cm × 2.6 cm) involving the subscapularis muscle and the lower angle of the scapula, confirming osteomyelitis in this segment. There was no evidence of dissemination elsewhere, and no joint involvement was noted. Percutaneous drainage of the abscess was suggested (Figs 1, 2).</p><p>The patient was transferred to a tertiary centre to assess the need for drainage, either percutaneously or surgically. A second MRI showed a significant reduction in abscess size. Consequently, the decision was made to continue with optimised parenteral antibiotic therapy (flucloxacillin 150 mg/kg/day and clindamycin 40 mg/kg/day), resulting in clinical improvement without surgical intervention.</p><p>After 2 weeks of parenteral therapy, the patient was discharged to complete a 4-week course of oral antibiotics. At the 6-month follow-up, he was pain-free with a full range of motion. Follow-up MRI showed complete resolution of the infection, with no features suggestive of ongoing osteomyelitis and only reactive lymph nodes in the left axilla. Blood tests were normal with leukocytes 5780/μL (neutrophils 1200/μL), C-reactive protein 0.12 mg/L and sedimentation rate 9 mm/h.</p><p>Scapular AHO is rare in the paediatric population, with abscess formation in the subscapularis muscle being even rarer.<span><sup>1-7</sup></span></p><p>While urgent surgical intervention combined with antibiotic therapy is typically recommended for abscess collections,<span><sup>2, 4, 5, 7</sup></span> this case demonstrates that conservative management with antibiotics alone can be effective. This approach may reduce complications such as surgical site infections and anaesthesia-related risks.</p><p>In our case, the decision for conservative treatment was based on the patient's clinical stability and rapid improvement with antibiotic therapy. The initial observation period prior to the second MRI was marked by significant clinical improvement, including the resolution of fever within 3 days and a decrease in inflammatory markers. Blood cultures repeated during the hospitalisation showed clearance of bacteremia. The second MRI, performed after 1 week of antibiotic therapy, demonstrated a significant reduction in abscess size and improvement in osteomyelitis features. The multidisciplinary team decided against surgical intervention due to the patient's rapid clinical improvement, the risks associated with surgery and anaesthesia in a young child, and the feasibility of continued close monitoring.</p><p>Throughout the 6-week antibiotic course, the patient's progress was monitored with weekly blood tests to track inflammatory markers and clinical examinations to assess symptoms. The chosen antibiotics for the oral phase included flucloxacillin (50 mg/kg/day) and clindamycin (30 mg/kg/day).</p><p>Conservative treatment of abscesses associated with osteomyelitis in other body areas has been documented, particularly in small abscesses with good antibiotic response.<span><sup>8, 9</sup></span> Potential complications that may be reduced with conservative therapy include surgical site infections, anaesthesia-related risks and prolonged hospital stays. Further research is needed to validate these findings and establish criteria for conservative management of similar cases.</p><p>This case underscores the importance of timely diagnosis and the potential efficacy of conservative therapy in treating subscapular abscesses. Future studies should involve larger sample sizes and longer follow-up periods to better understand the long-term outcomes of conservative therapy for subscapular abscess. Additionally, identifying patient characteristics that may predict better responses to conservative approaches, such as infection type and location, patient age, underlying medical conditions and risk factors for treatment failure, could guide treatment decisions and improve patient outcomes.</p>","PeriodicalId":16648,"journal":{"name":"Journal of paediatrics and child health","volume":"60 12","pages":"887-888"},"PeriodicalIF":1.4000,"publicationDate":"2024-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16695","citationCount":"0","resultStr":"{\"title\":\"Acute hematogenous osteomyelitis of the scapula complicated with a subscapular abscess: First described case of a conservative approach\",\"authors\":\"Joana F. Pires, Sara Geraldes Paulino, Daniela Araújo, Francisco Miranda Antunes, Isabel Martinho\",\"doi\":\"10.1111/jpc.16695\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A previously healthy 3-year-old boy presented to the ED in May 2022 with pain and functional impairment of the left upper limb following a fall the previous day. The patient developed a fever while in the ED, with a peak temperature of 39°C noted during the initial physical examination. His physical examination revealed limited movement and pain in the left shoulder, with no skin lesions. Vital signs included a temperature of 39°C, heart rate of 115 bpm, respiratory rate of 20 breaths per minute, blood pressure of 98/53 mmHg and oxygen saturation of 100% on room air.</p><p>Initial diagnostic imaging, including plain radiography and ultrasound of the left shoulder, revealed no abnormalities. Laboratory results showed leukocytes 16 660/μL (neutrophils 15 000/μL), C-reactive protein 14.25 mg/L and sedimentation rate 54 mm/h. The patient was hospitalised with empirical intravenous cefuroxime (150 mg/kg/day) due to suspicion of osteoarticular infection. Blood cultures later grew methicillin-sensitive Staphylococcus aureus (MSSA), and treatment was adjusted to intravenous flucloxacillin (150 mg/kg/day).</p><p>MRI on the fourth day of hospitalisation revealed a large multiloculated abscess (6 cm × 4 cm × 2.6 cm) involving the subscapularis muscle and the lower angle of the scapula, confirming osteomyelitis in this segment. There was no evidence of dissemination elsewhere, and no joint involvement was noted. Percutaneous drainage of the abscess was suggested (Figs 1, 2).</p><p>The patient was transferred to a tertiary centre to assess the need for drainage, either percutaneously or surgically. A second MRI showed a significant reduction in abscess size. Consequently, the decision was made to continue with optimised parenteral antibiotic therapy (flucloxacillin 150 mg/kg/day and clindamycin 40 mg/kg/day), resulting in clinical improvement without surgical intervention.</p><p>After 2 weeks of parenteral therapy, the patient was discharged to complete a 4-week course of oral antibiotics. At the 6-month follow-up, he was pain-free with a full range of motion. Follow-up MRI showed complete resolution of the infection, with no features suggestive of ongoing osteomyelitis and only reactive lymph nodes in the left axilla. Blood tests were normal with leukocytes 5780/μL (neutrophils 1200/μL), C-reactive protein 0.12 mg/L and sedimentation rate 9 mm/h.</p><p>Scapular AHO is rare in the paediatric population, with abscess formation in the subscapularis muscle being even rarer.<span><sup>1-7</sup></span></p><p>While urgent surgical intervention combined with antibiotic therapy is typically recommended for abscess collections,<span><sup>2, 4, 5, 7</sup></span> this case demonstrates that conservative management with antibiotics alone can be effective. This approach may reduce complications such as surgical site infections and anaesthesia-related risks.</p><p>In our case, the decision for conservative treatment was based on the patient's clinical stability and rapid improvement with antibiotic therapy. The initial observation period prior to the second MRI was marked by significant clinical improvement, including the resolution of fever within 3 days and a decrease in inflammatory markers. Blood cultures repeated during the hospitalisation showed clearance of bacteremia. The second MRI, performed after 1 week of antibiotic therapy, demonstrated a significant reduction in abscess size and improvement in osteomyelitis features. The multidisciplinary team decided against surgical intervention due to the patient's rapid clinical improvement, the risks associated with surgery and anaesthesia in a young child, and the feasibility of continued close monitoring.</p><p>Throughout the 6-week antibiotic course, the patient's progress was monitored with weekly blood tests to track inflammatory markers and clinical examinations to assess symptoms. The chosen antibiotics for the oral phase included flucloxacillin (50 mg/kg/day) and clindamycin (30 mg/kg/day).</p><p>Conservative treatment of abscesses associated with osteomyelitis in other body areas has been documented, particularly in small abscesses with good antibiotic response.<span><sup>8, 9</sup></span> Potential complications that may be reduced with conservative therapy include surgical site infections, anaesthesia-related risks and prolonged hospital stays. Further research is needed to validate these findings and establish criteria for conservative management of similar cases.</p><p>This case underscores the importance of timely diagnosis and the potential efficacy of conservative therapy in treating subscapular abscesses. Future studies should involve larger sample sizes and longer follow-up periods to better understand the long-term outcomes of conservative therapy for subscapular abscess. Additionally, identifying patient characteristics that may predict better responses to conservative approaches, such as infection type and location, patient age, underlying medical conditions and risk factors for treatment failure, could guide treatment decisions and improve patient outcomes.</p>\",\"PeriodicalId\":16648,\"journal\":{\"name\":\"Journal of paediatrics and child health\",\"volume\":\"60 12\",\"pages\":\"887-888\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-10-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jpc.16695\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of paediatrics and child health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16695\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of paediatrics and child health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jpc.16695","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Acute hematogenous osteomyelitis of the scapula complicated with a subscapular abscess: First described case of a conservative approach
A previously healthy 3-year-old boy presented to the ED in May 2022 with pain and functional impairment of the left upper limb following a fall the previous day. The patient developed a fever while in the ED, with a peak temperature of 39°C noted during the initial physical examination. His physical examination revealed limited movement and pain in the left shoulder, with no skin lesions. Vital signs included a temperature of 39°C, heart rate of 115 bpm, respiratory rate of 20 breaths per minute, blood pressure of 98/53 mmHg and oxygen saturation of 100% on room air.
Initial diagnostic imaging, including plain radiography and ultrasound of the left shoulder, revealed no abnormalities. Laboratory results showed leukocytes 16 660/μL (neutrophils 15 000/μL), C-reactive protein 14.25 mg/L and sedimentation rate 54 mm/h. The patient was hospitalised with empirical intravenous cefuroxime (150 mg/kg/day) due to suspicion of osteoarticular infection. Blood cultures later grew methicillin-sensitive Staphylococcus aureus (MSSA), and treatment was adjusted to intravenous flucloxacillin (150 mg/kg/day).
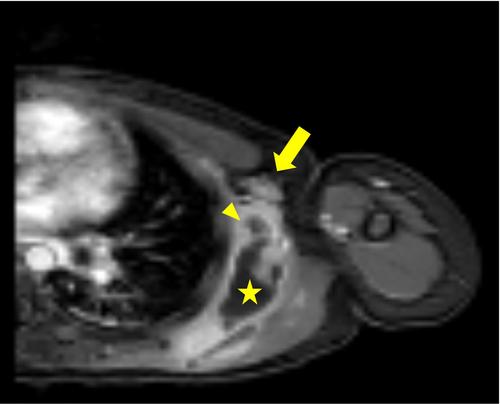
MRI on the fourth day of hospitalisation revealed a large multiloculated abscess (6 cm × 4 cm × 2.6 cm) involving the subscapularis muscle and the lower angle of the scapula, confirming osteomyelitis in this segment. There was no evidence of dissemination elsewhere, and no joint involvement was noted. Percutaneous drainage of the abscess was suggested (Figs 1, 2).
The patient was transferred to a tertiary centre to assess the need for drainage, either percutaneously or surgically. A second MRI showed a significant reduction in abscess size. Consequently, the decision was made to continue with optimised parenteral antibiotic therapy (flucloxacillin 150 mg/kg/day and clindamycin 40 mg/kg/day), resulting in clinical improvement without surgical intervention.
After 2 weeks of parenteral therapy, the patient was discharged to complete a 4-week course of oral antibiotics. At the 6-month follow-up, he was pain-free with a full range of motion. Follow-up MRI showed complete resolution of the infection, with no features suggestive of ongoing osteomyelitis and only reactive lymph nodes in the left axilla. Blood tests were normal with leukocytes 5780/μL (neutrophils 1200/μL), C-reactive protein 0.12 mg/L and sedimentation rate 9 mm/h.
Scapular AHO is rare in the paediatric population, with abscess formation in the subscapularis muscle being even rarer.1-7
While urgent surgical intervention combined with antibiotic therapy is typically recommended for abscess collections,2, 4, 5, 7 this case demonstrates that conservative management with antibiotics alone can be effective. This approach may reduce complications such as surgical site infections and anaesthesia-related risks.
In our case, the decision for conservative treatment was based on the patient's clinical stability and rapid improvement with antibiotic therapy. The initial observation period prior to the second MRI was marked by significant clinical improvement, including the resolution of fever within 3 days and a decrease in inflammatory markers. Blood cultures repeated during the hospitalisation showed clearance of bacteremia. The second MRI, performed after 1 week of antibiotic therapy, demonstrated a significant reduction in abscess size and improvement in osteomyelitis features. The multidisciplinary team decided against surgical intervention due to the patient's rapid clinical improvement, the risks associated with surgery and anaesthesia in a young child, and the feasibility of continued close monitoring.
Throughout the 6-week antibiotic course, the patient's progress was monitored with weekly blood tests to track inflammatory markers and clinical examinations to assess symptoms. The chosen antibiotics for the oral phase included flucloxacillin (50 mg/kg/day) and clindamycin (30 mg/kg/day).
Conservative treatment of abscesses associated with osteomyelitis in other body areas has been documented, particularly in small abscesses with good antibiotic response.8, 9 Potential complications that may be reduced with conservative therapy include surgical site infections, anaesthesia-related risks and prolonged hospital stays. Further research is needed to validate these findings and establish criteria for conservative management of similar cases.
This case underscores the importance of timely diagnosis and the potential efficacy of conservative therapy in treating subscapular abscesses. Future studies should involve larger sample sizes and longer follow-up periods to better understand the long-term outcomes of conservative therapy for subscapular abscess. Additionally, identifying patient characteristics that may predict better responses to conservative approaches, such as infection type and location, patient age, underlying medical conditions and risk factors for treatment failure, could guide treatment decisions and improve patient outcomes.
期刊介绍:
The Journal of Paediatrics and Child Health publishes original research articles of scientific excellence in paediatrics and child health. Research Articles, Case Reports and Letters to the Editor are published, together with invited Reviews, Annotations, Editorial Comments and manuscripts of educational interest.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
