Aqib H Zehri, Rebecca L Calafiore, Keyan A Peterson, Carol A Kittel, Jed A Osei, Jonathan L Wilson, Wesley Hsu
{"title":"脊柱多发性骨髓瘤的手术治疗:全国住院病人抽样数据库的启示。","authors":"Aqib H Zehri, Rebecca L Calafiore, Keyan A Peterson, Carol A Kittel, Jed A Osei, Jonathan L Wilson, Wesley Hsu","doi":"10.21037/jss-24-54","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Management of multiple myeloma (MM) of the spine includes a multimodal approach consisting of chemotherapy, bisphosphonates, radiation, and surgical intervention. This study aims to explore the trends in surgical treatment of MM including hospital costs, odds of complications, and the impact of patient comorbidities on the risk of complications using the National Inpatient Sample (NIS) database.</p><p><strong>Methods: </strong>The NIS was queried for patients with MM and plasmacytoma of the spine who underwent surgical intervention between 2005 and 2014. Rates of spinal decompression, spinal stabilization with or without decompression, and vertebral augmentation were analyzed. The effect of various patient characteristics on outcome was analyzed by multivariate analysis and stratified by surgical procedure.</p><p><strong>Results: </strong>Vertebral augmentation (9,643, 65.7%) was the most commonly performed procedure, followed by spinal stabilization with or without decompression (4,176, 28.4%) and then decompression alone (868, 5.9%). The total population-adjusted rate of surgical management for MM remained stable during the study period, while the rate of spinal stabilization increased (P<0.001) and the rate of vertebral augmentation decreased (P=0.01). Vertebral augmentation was associated with shorter inpatient hospital stay, lower total cost, and higher likelihood of discharging to home. The complication rate increased over time for vertebral augmentation procedures (P<0.001) while spinal stabilization and decompression complication rates remained stable. The complication rate for all procedures was higher in male patients (P<0.001) and increased with the number of patient comorbidities (P<0.001).</p><p><strong>Conclusions: </strong>Spinal surgery seems to be increasing for the management of spinal MM in the inpatient setting, while the rate of vertebral augmentation is decreasing. Vertebroplasty and similar palliative procedures may continue to decrease as advancements in surgical technology and technique allow for safer surgical intervention. The decision to employ aggressive surgical intervention, however, must always take into account the patient's comorbidities, overall systemic disease burden, and the potential for significant enhancement in meaningful clinical outcome.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"10 3","pages":"428-437"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467281/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical management of spinal multiple myeloma: insights from the National Inpatient Sample database.\",\"authors\":\"Aqib H Zehri, Rebecca L Calafiore, Keyan A Peterson, Carol A Kittel, Jed A Osei, Jonathan L Wilson, Wesley Hsu\",\"doi\":\"10.21037/jss-24-54\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Management of multiple myeloma (MM) of the spine includes a multimodal approach consisting of chemotherapy, bisphosphonates, radiation, and surgical intervention. This study aims to explore the trends in surgical treatment of MM including hospital costs, odds of complications, and the impact of patient comorbidities on the risk of complications using the National Inpatient Sample (NIS) database.</p><p><strong>Methods: </strong>The NIS was queried for patients with MM and plasmacytoma of the spine who underwent surgical intervention between 2005 and 2014. Rates of spinal decompression, spinal stabilization with or without decompression, and vertebral augmentation were analyzed. The effect of various patient characteristics on outcome was analyzed by multivariate analysis and stratified by surgical procedure.</p><p><strong>Results: </strong>Vertebral augmentation (9,643, 65.7%) was the most commonly performed procedure, followed by spinal stabilization with or without decompression (4,176, 28.4%) and then decompression alone (868, 5.9%). The total population-adjusted rate of surgical management for MM remained stable during the study period, while the rate of spinal stabilization increased (P<0.001) and the rate of vertebral augmentation decreased (P=0.01). Vertebral augmentation was associated with shorter inpatient hospital stay, lower total cost, and higher likelihood of discharging to home. The complication rate increased over time for vertebral augmentation procedures (P<0.001) while spinal stabilization and decompression complication rates remained stable. The complication rate for all procedures was higher in male patients (P<0.001) and increased with the number of patient comorbidities (P<0.001).</p><p><strong>Conclusions: </strong>Spinal surgery seems to be increasing for the management of spinal MM in the inpatient setting, while the rate of vertebral augmentation is decreasing. Vertebroplasty and similar palliative procedures may continue to decrease as advancements in surgical technology and technique allow for safer surgical intervention. The decision to employ aggressive surgical intervention, however, must always take into account the patient's comorbidities, overall systemic disease burden, and the potential for significant enhancement in meaningful clinical outcome.</p>\",\"PeriodicalId\":17131,\"journal\":{\"name\":\"Journal of spine surgery\",\"volume\":\"10 3\",\"pages\":\"428-437\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467281/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of spine surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/jss-24-54\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-54","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:脊柱多发性骨髓瘤(MM)的治疗包括化疗、双磷酸盐、放疗和手术干预等多模式方法。本研究旨在利用全国住院病人抽样调查(NIS)数据库探讨多发性骨髓瘤手术治疗的趋势,包括住院费用、并发症几率以及患者合并症对并发症风险的影响:方法:对 2005 年至 2014 年期间接受手术治疗的 MM 和脊柱浆细胞瘤患者进行了 NIS 查询。分析了脊柱减压率、有或无减压的脊柱稳定率以及椎体增强率。通过多变量分析和手术方法分层分析了患者的各种特征对结果的影响:结果:椎体增强术(9643例,65.7%)是最常见的手术,其次是脊柱稳定加或不加减压术(4176例,28.4%),然后是单纯减压术(868例,5.9%)。在研究期间,经人口调整后的MM手术治疗总比率保持稳定,而脊柱稳定术的比率则有所上升(PC结论:在住院治疗脊柱MM的过程中,脊柱手术的比例似乎在上升,而椎体增强手术的比例却在下降。随着手术技术和技巧的进步,手术干预更加安全,椎体成形术和类似的姑息性手术可能会继续减少。但是,在决定是否采用积极的手术干预时,必须始终考虑患者的合并症、全身疾病负担以及显著改善有意义的临床结果的潜力。
Surgical management of spinal multiple myeloma: insights from the National Inpatient Sample database.
Background: Management of multiple myeloma (MM) of the spine includes a multimodal approach consisting of chemotherapy, bisphosphonates, radiation, and surgical intervention. This study aims to explore the trends in surgical treatment of MM including hospital costs, odds of complications, and the impact of patient comorbidities on the risk of complications using the National Inpatient Sample (NIS) database.
Methods: The NIS was queried for patients with MM and plasmacytoma of the spine who underwent surgical intervention between 2005 and 2014. Rates of spinal decompression, spinal stabilization with or without decompression, and vertebral augmentation were analyzed. The effect of various patient characteristics on outcome was analyzed by multivariate analysis and stratified by surgical procedure.
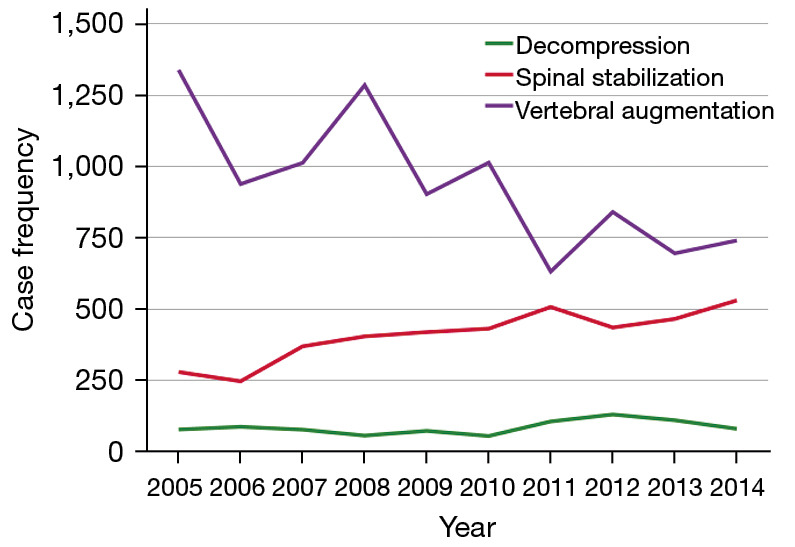
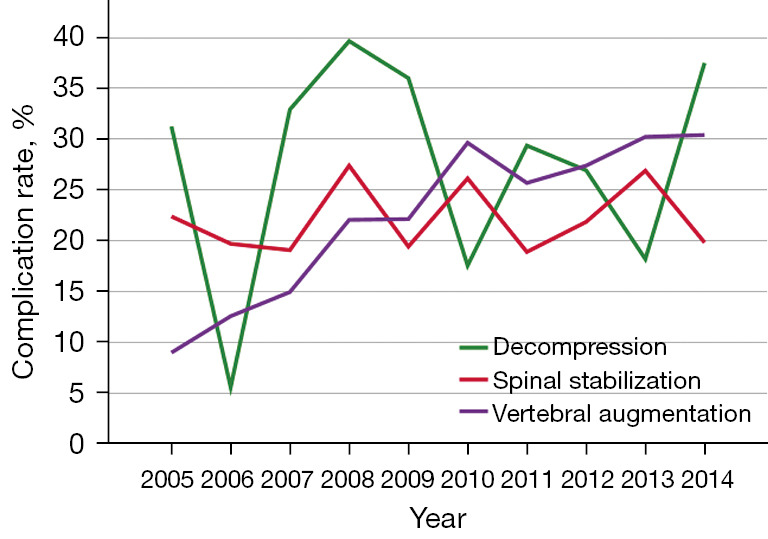
Results: Vertebral augmentation (9,643, 65.7%) was the most commonly performed procedure, followed by spinal stabilization with or without decompression (4,176, 28.4%) and then decompression alone (868, 5.9%). The total population-adjusted rate of surgical management for MM remained stable during the study period, while the rate of spinal stabilization increased (P<0.001) and the rate of vertebral augmentation decreased (P=0.01). Vertebral augmentation was associated with shorter inpatient hospital stay, lower total cost, and higher likelihood of discharging to home. The complication rate increased over time for vertebral augmentation procedures (P<0.001) while spinal stabilization and decompression complication rates remained stable. The complication rate for all procedures was higher in male patients (P<0.001) and increased with the number of patient comorbidities (P<0.001).
Conclusions: Spinal surgery seems to be increasing for the management of spinal MM in the inpatient setting, while the rate of vertebral augmentation is decreasing. Vertebroplasty and similar palliative procedures may continue to decrease as advancements in surgical technology and technique allow for safer surgical intervention. The decision to employ aggressive surgical intervention, however, must always take into account the patient's comorbidities, overall systemic disease burden, and the potential for significant enhancement in meaningful clinical outcome.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
