Diogo Lino Moura, Helena Sofia Pais, Paulo Lourenço, Carlos Jardim
{"title":"创伤后椎体骨坏死的手术治疗(包括椎体内膨胀性植入物)--临床、功能和影像学结果以及7年来的中心经验。","authors":"Diogo Lino Moura, Helena Sofia Pais, Paulo Lourenço, Carlos Jardim","doi":"10.21037/jss-24-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The effective treatment of post-traumatic vertebral osteonecrosis continues to be an under discussion and controversial subject. Armed kyphoplasty with expansive intravertebral implants is an emerging procedure, which, in theory, allow for a more effective preservation of the restored vertebral height. The development of the indications for these recent devices has given rise to auspicious outcomes in vertebral non-union situations. The aim of this study is to evaluate the clinical, functional and imaging outcomes of the surgical treatment of situations of post-traumatic vertebral necrosis, following a therapeutic algorithm that includes armed kyphoplasty with intravertebral expansive implants and bridge pedicular stabilization, according to a predefined necrosis stage.</p><p><strong>Methods: </strong>We present a retrospective observational study, in which 35 patients took part, including a total of 35 cases of post-traumatic vertebral osteonecrosis submitted to surgical treatment over 7 years (between 2016 and 2023) at the same center according to a defined therapeutic algorithm. The cases were staged according to vertebral morphology (non-plana or plana) and mobility (mobile or immobile)-stages 1m (mobile necrotic vertebra non-plana), 1i (immobile necrotic vertebra non-plana), 2m (mobile necrotic vertebra plana), and 2i (immobile necrotic vertebra plana)-and the following surgeries were performed: armed kyphoplasty with intravertebral expansive implants filled with bone cement, associated or not to adjacent pedicle instrumentation; or bridge pedicle fixation of the adjacent levels. Clinical results [Patient Global Impression of Change (PGIC), Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI)] as well as imaging outcomes (restoration and preservation of the heights of the vertebral body) were studied. The mean follow-up time corresponded to 3.17 years (range, 1-7.5 years).</p><p><strong>Results: </strong>Most of the clinical-functional and imaging parameters showed important improvements after surgical treatment, with few complications. A statistically significant greater degree of functional improvement was found in plana vertebrae when compared to non-plana, which reflects that the first are quite symptomatic and disabling at the beginning and improve a lot with surgical treatment. Significant indirect correlations were found between the time from the initial fracture to surgical intervention after diagnosis of vertebral necrosis and the anterior sagittal height in the immediate postoperative time and at the ending of the follow-up. Also, a significant direct correlation was identified between this time and the VAS for pain at the end of the follow-up and the PGIC scale in the same period. It was also found that patients with surgical complications had a statistically significantly longer time between the initial fracture and surgery for post-traumatic necrosis.</p><p><strong>Conclusions: </strong>We present the results of a surgical therapeutic algorithm that includes the use of recent expansive intravertebral implants at post-traumatic vertebral osteonecrosis, resulting in satisfactory clinical, functional and imaging results. This work shows a pioneering statistical demonstration of the clinical, functional and imaging importance of early detection of this condition (ideally in vertebrae non-plana morphology stages), so that there is still sufficient bone tissue in the vertebral body to permit the stabilization and restoration of its anatomy through a minimally invasive interior reconstruction, with percutaneous access and quicker convalescence, that is to say, armed kyphoplasty, avoiding the unwanted disease progression that will require more aggressive surgical solutions that doesn't allow anatomical restauration.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"10 3","pages":"450-467"},"PeriodicalIF":2.3000,"publicationDate":"2024-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467275/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical treatment of post-traumatic vertebral osteonecrosis including intravertebral expansive implants-clinical, functional and imaging outcomes and a center experience over 7 years.\",\"authors\":\"Diogo Lino Moura, Helena Sofia Pais, Paulo Lourenço, Carlos Jardim\",\"doi\":\"10.21037/jss-24-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The effective treatment of post-traumatic vertebral osteonecrosis continues to be an under discussion and controversial subject. Armed kyphoplasty with expansive intravertebral implants is an emerging procedure, which, in theory, allow for a more effective preservation of the restored vertebral height. The development of the indications for these recent devices has given rise to auspicious outcomes in vertebral non-union situations. The aim of this study is to evaluate the clinical, functional and imaging outcomes of the surgical treatment of situations of post-traumatic vertebral necrosis, following a therapeutic algorithm that includes armed kyphoplasty with intravertebral expansive implants and bridge pedicular stabilization, according to a predefined necrosis stage.</p><p><strong>Methods: </strong>We present a retrospective observational study, in which 35 patients took part, including a total of 35 cases of post-traumatic vertebral osteonecrosis submitted to surgical treatment over 7 years (between 2016 and 2023) at the same center according to a defined therapeutic algorithm. The cases were staged according to vertebral morphology (non-plana or plana) and mobility (mobile or immobile)-stages 1m (mobile necrotic vertebra non-plana), 1i (immobile necrotic vertebra non-plana), 2m (mobile necrotic vertebra plana), and 2i (immobile necrotic vertebra plana)-and the following surgeries were performed: armed kyphoplasty with intravertebral expansive implants filled with bone cement, associated or not to adjacent pedicle instrumentation; or bridge pedicle fixation of the adjacent levels. Clinical results [Patient Global Impression of Change (PGIC), Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI)] as well as imaging outcomes (restoration and preservation of the heights of the vertebral body) were studied. The mean follow-up time corresponded to 3.17 years (range, 1-7.5 years).</p><p><strong>Results: </strong>Most of the clinical-functional and imaging parameters showed important improvements after surgical treatment, with few complications. A statistically significant greater degree of functional improvement was found in plana vertebrae when compared to non-plana, which reflects that the first are quite symptomatic and disabling at the beginning and improve a lot with surgical treatment. Significant indirect correlations were found between the time from the initial fracture to surgical intervention after diagnosis of vertebral necrosis and the anterior sagittal height in the immediate postoperative time and at the ending of the follow-up. Also, a significant direct correlation was identified between this time and the VAS for pain at the end of the follow-up and the PGIC scale in the same period. It was also found that patients with surgical complications had a statistically significantly longer time between the initial fracture and surgery for post-traumatic necrosis.</p><p><strong>Conclusions: </strong>We present the results of a surgical therapeutic algorithm that includes the use of recent expansive intravertebral implants at post-traumatic vertebral osteonecrosis, resulting in satisfactory clinical, functional and imaging results. This work shows a pioneering statistical demonstration of the clinical, functional and imaging importance of early detection of this condition (ideally in vertebrae non-plana morphology stages), so that there is still sufficient bone tissue in the vertebral body to permit the stabilization and restoration of its anatomy through a minimally invasive interior reconstruction, with percutaneous access and quicker convalescence, that is to say, armed kyphoplasty, avoiding the unwanted disease progression that will require more aggressive surgical solutions that doesn't allow anatomical restauration.</p>\",\"PeriodicalId\":17131,\"journal\":{\"name\":\"Journal of spine surgery\",\"volume\":\"10 3\",\"pages\":\"450-467\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467275/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of spine surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/jss-24-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:创伤后椎体骨坏死的有效治疗仍是一个讨论和争议的话题。使用膨胀性椎体内植入物进行武装椎体成形术是一种新兴的治疗方法,理论上可以更有效地保留恢复后的椎体高度。随着这些新设备适应症的发展,在椎体不愈合情况下取得了良好的效果。本研究的目的是根据预先确定的坏死分期,评估创伤后椎体坏死情况下手术治疗的临床、功能和影像学结果:我们进行了一项回顾性观察研究,共有35名患者参与其中,包括7年间(2016年至2023年)在同一中心接受手术治疗的35例创伤后椎体骨坏死病例,这些病例都是按照既定的治疗算法进行治疗的。根据椎体形态(非椎体或椎体平面)和活动度(活动或不活动)对病例进行分期--1m期(活动坏死椎体非椎体平面)、1i期(不活动坏死椎体非椎体平面)、2m期(活动坏死椎体平面)和2i期(不活动坏死椎体平面)--并进行了以下手术:椎体内膨胀性植入物填充骨水泥的武装椎体成形术,与邻近椎弓根器械相关或无关;或邻近水平的桥式椎弓根固定术。对临床结果[患者整体变化印象(PGIC)、视觉模拟量表(VAS)和Oswestry残疾指数(ODI)]以及影像学结果(椎体高度的恢复和保留)进行了研究。平均随访时间为 3.17 年(1-7.5 年不等):结果:手术治疗后,大多数临床功能和影像学参数都有明显改善,并发症很少。与非平面椎体相比,平面椎体的功能改善程度在统计学上更为明显,这反映出平面椎体在初期症状较重、致残率较高,手术治疗后症状会得到很大改善。从最初骨折到确诊椎体坏死后进行手术治疗的时间与术后即刻和随访结束时的前矢状面高度之间存在显著的间接相关性。此外,该时间与随访结束时的疼痛 VAS 值和同期的 PGIC 量表之间也存在明显的直接相关性。研究还发现,有手术并发症的患者从初次骨折到创伤后坏死手术之间的时间明显更长:我们介绍了一种手术治疗算法的结果,该算法包括在创伤后椎体骨坏死中使用最新的膨胀性椎体内植入物,从而获得令人满意的临床、功能和影像学效果。这项工作以开创性的统计方法证明了早期发现这种病症(最好是在椎体非plana形态阶段)在临床、功能和影像学方面的重要性,这样椎体内仍有足够的骨组织,可以通过经皮入路的微创内部重建和更快的康复来稳定和恢复椎体解剖结构,也就是说,可以通过武装椎体成形术来避免不必要的疾病进展,因为疾病进展需要更激进的手术方案,而这种手术方案无法恢复椎体解剖结构。
Surgical treatment of post-traumatic vertebral osteonecrosis including intravertebral expansive implants-clinical, functional and imaging outcomes and a center experience over 7 years.
Background: The effective treatment of post-traumatic vertebral osteonecrosis continues to be an under discussion and controversial subject. Armed kyphoplasty with expansive intravertebral implants is an emerging procedure, which, in theory, allow for a more effective preservation of the restored vertebral height. The development of the indications for these recent devices has given rise to auspicious outcomes in vertebral non-union situations. The aim of this study is to evaluate the clinical, functional and imaging outcomes of the surgical treatment of situations of post-traumatic vertebral necrosis, following a therapeutic algorithm that includes armed kyphoplasty with intravertebral expansive implants and bridge pedicular stabilization, according to a predefined necrosis stage.
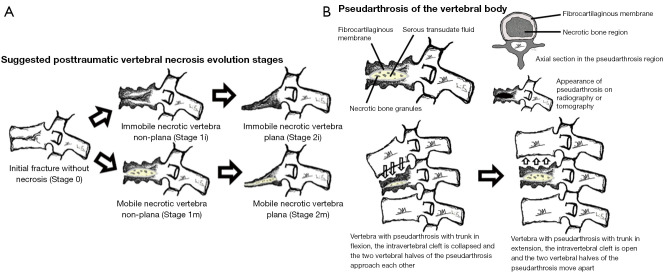
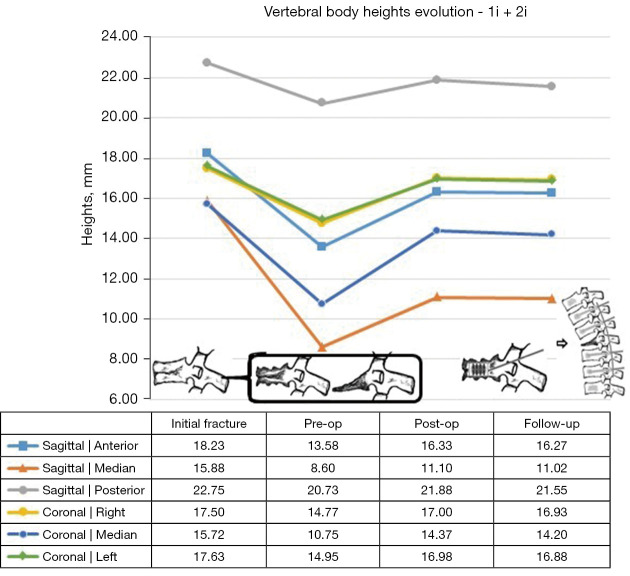
Methods: We present a retrospective observational study, in which 35 patients took part, including a total of 35 cases of post-traumatic vertebral osteonecrosis submitted to surgical treatment over 7 years (between 2016 and 2023) at the same center according to a defined therapeutic algorithm. The cases were staged according to vertebral morphology (non-plana or plana) and mobility (mobile or immobile)-stages 1m (mobile necrotic vertebra non-plana), 1i (immobile necrotic vertebra non-plana), 2m (mobile necrotic vertebra plana), and 2i (immobile necrotic vertebra plana)-and the following surgeries were performed: armed kyphoplasty with intravertebral expansive implants filled with bone cement, associated or not to adjacent pedicle instrumentation; or bridge pedicle fixation of the adjacent levels. Clinical results [Patient Global Impression of Change (PGIC), Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI)] as well as imaging outcomes (restoration and preservation of the heights of the vertebral body) were studied. The mean follow-up time corresponded to 3.17 years (range, 1-7.5 years).
Results: Most of the clinical-functional and imaging parameters showed important improvements after surgical treatment, with few complications. A statistically significant greater degree of functional improvement was found in plana vertebrae when compared to non-plana, which reflects that the first are quite symptomatic and disabling at the beginning and improve a lot with surgical treatment. Significant indirect correlations were found between the time from the initial fracture to surgical intervention after diagnosis of vertebral necrosis and the anterior sagittal height in the immediate postoperative time and at the ending of the follow-up. Also, a significant direct correlation was identified between this time and the VAS for pain at the end of the follow-up and the PGIC scale in the same period. It was also found that patients with surgical complications had a statistically significantly longer time between the initial fracture and surgery for post-traumatic necrosis.
Conclusions: We present the results of a surgical therapeutic algorithm that includes the use of recent expansive intravertebral implants at post-traumatic vertebral osteonecrosis, resulting in satisfactory clinical, functional and imaging results. This work shows a pioneering statistical demonstration of the clinical, functional and imaging importance of early detection of this condition (ideally in vertebrae non-plana morphology stages), so that there is still sufficient bone tissue in the vertebral body to permit the stabilization and restoration of its anatomy through a minimally invasive interior reconstruction, with percutaneous access and quicker convalescence, that is to say, armed kyphoplasty, avoiding the unwanted disease progression that will require more aggressive surgical solutions that doesn't allow anatomical restauration.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
