Jacob Fry, Angie Bone, Keiichiro Kanemoto, Carolynn L Smith, Nick Watts
{"title":"医疗保健中的环境足迹:入门指南。","authors":"Jacob Fry, Angie Bone, Keiichiro Kanemoto, Carolynn L Smith, Nick Watts","doi":"10.5694/mja2.52481","DOIUrl":null,"url":null,"abstract":"<p>Health care systems are responsible for 4–5% of global greenhouse gas (GHG) emissions.<span><sup>1, 2</sup></span> There is increasing pressure to reduce the environmental effects of health care as more health professionals recognise its contribution to climate change.<span><sup>3, 4</sup></span> However, measuring environmental effects and assessing progress towards decarbonisation are not trivial processes because the mechanisms driving environmental burdens are often hidden. Although much of the early focus in health has been on decarbonisation of building and transport assets, most of health care's GHG emissions occur within the supply chains that provision the health care system before the final delivery of services.<span><sup>5</sup></span></p><p>This article is intended to serve as a beginner's introduction to the environmental footprinting techniques that can be applied to uncover health care's environmental impacts, including impacts occurring along supply chains. This article focuses on GHG emissions, but many other pollutants and environmental stressors can be assessed using these methods.</p><p>Environmental impacts can be separated into “direct” and “indirect” impacts. Direct impacts occur within an organisation's physical boundary, for example hospital grounds. Indirect impacts occur outside this immediate boundary, for example impacts from purchased products. Direct impacts are relatively easy to estimate using fossil fuel consumption and utility bills. In contrast, estimating indirect emissions is more challenging for health care organisations and requires detailed data on the quantity or cost of procured products and services and the application of environmental footprinting techniques. An organisation's indirect emissions form part of their suppliers’ direct emissions and likely occur in other regions and jurisdictions, rendering them more abstract and intangible.</p><p>Quantifying indirect environmental impacts requires consideration of the supply chains delivering goods and services to final consumption. Supply chains link production layers together, where at each stage numerous inputs and components are combined to make intermediate products. This can be depicted as a tree branching upwards and outwards from the consumer, with each node representing a production stage (Box 1). Here, “upstream” refers to layers occurring before the product reaches a consumer, and “downstream” refers to layers after final consumption, including disposal of the product.</p><p>Environmental effects can occur at each layer and accumulate along the supply chain as more layers are included.<span><sup>6</sup></span> Eventually, supply chains reach consumers as final products. Accounting for all upstream environmental impacts associated with a product or service is onerous because of the large number of production layers and the many inputs into each layer. An illustrative example of supply chain is “fossil fuel combustion > petrochemical refining > plastic sample jars > pathology services”, which is just one of the many supply chains contributing to “pathology services”.<span><sup>7</sup></span></p><p>The “system boundary” is a conceptual limit within which environmental effects are captured by an assessment method.<span><sup>8</sup></span> The boundary is considered “incomplete” when all important activities are not within the boundary, resulting in some fraction of environmental effects being uncounted.<span><sup>9</sup></span> An awareness of the defined system boundary is important when calculating the full environmental footprint of a product or process and when making comparisons. The extent to which unaccounted impacts are significant depends on the process and activity and may include, for example, impacts arising from capital works, infrastructure and the services sector. Box 2 depicts the system boundary in relation to final consumption and intermediate production stages.</p><p>Although in common use, these scopes are a simplification and do not always neatly align with organisation structure or function. For example, emissions from ambulatory patient transport may be attributed to a health system's scope 1 emissions; however, patient self-transport emissions remain uncounted. In addition, the scope framework does not consider shared responsibility of emissions between upstream and downstream actors in the supply chain. These difficulties reflect wider societal complexities in attributing responsibility for emissions reductions.<span><sup>11</sup></span></p><p>Two main environmental footprinting methods can be distinguished: life cycle assessment (LCA) and environmentally extended input–output analysis (EE-IOA).</p><p>Which assessment technique should be used depends on the health care context and research question. In general, questions involving diagnostic methods and treatments are best answered using LCA techniques, whereas assessing overall progress at the health system level is more suited to EE-IOA. International Organization for Standardization (ISO) 14040:2006 and 14044:2006 provide guidelines to practitioners doing life cycle assessments. The European Union is introducing new regulations to combat greenwashing<span><sup>26</sup></span> and has its own guidelines on how LCAs should be done.<span><sup>27</sup></span> IOA and its extensions are also governed by global standards.<span><sup>28</sup></span> Adherence to these standards and guidelines can provide an indication of the quality and trustworthiness of sustainability assessments and enables comparison between studies.</p><p>Environmental impacts will increasingly need to be assessed and considered as part of health sector decision making at every level. However, systems for environmental data collection, storage and analysis are often limited in many health systems and usually not standardised or linked to clinical and population outcomes.<span><sup>29</sup></span> Information about product environmental performance is rarely provided by manufacturers, and the underlying data are often inaccessible.<span><sup>30</sup></span></p><p>Health care professionals have an important role in normalising consideration of the environmental impact of health care and advocating for availability of evidence and the supporting infrastructure to evaluate and reduce that impact. We are not suggesting that environmental footprinting is the primary role of health care workers, nor are we suggesting that considerations of environmental impact should take precedence over clinical outcomes. Rather, environmental sustainability should be considered as a dimension of quality, safety and good governance alongside patient and population health outcomes.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 9","pages":"464-467"},"PeriodicalIF":8.5000,"publicationDate":"2024-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52481","citationCount":"0","resultStr":"{\"title\":\"Environmental footprinting in health care: a primer\",\"authors\":\"Jacob Fry, Angie Bone, Keiichiro Kanemoto, Carolynn L Smith, Nick Watts\",\"doi\":\"10.5694/mja2.52481\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Health care systems are responsible for 4–5% of global greenhouse gas (GHG) emissions.<span><sup>1, 2</sup></span> There is increasing pressure to reduce the environmental effects of health care as more health professionals recognise its contribution to climate change.<span><sup>3, 4</sup></span> However, measuring environmental effects and assessing progress towards decarbonisation are not trivial processes because the mechanisms driving environmental burdens are often hidden. Although much of the early focus in health has been on decarbonisation of building and transport assets, most of health care's GHG emissions occur within the supply chains that provision the health care system before the final delivery of services.<span><sup>5</sup></span></p><p>This article is intended to serve as a beginner's introduction to the environmental footprinting techniques that can be applied to uncover health care's environmental impacts, including impacts occurring along supply chains. This article focuses on GHG emissions, but many other pollutants and environmental stressors can be assessed using these methods.</p><p>Environmental impacts can be separated into “direct” and “indirect” impacts. Direct impacts occur within an organisation's physical boundary, for example hospital grounds. Indirect impacts occur outside this immediate boundary, for example impacts from purchased products. Direct impacts are relatively easy to estimate using fossil fuel consumption and utility bills. In contrast, estimating indirect emissions is more challenging for health care organisations and requires detailed data on the quantity or cost of procured products and services and the application of environmental footprinting techniques. An organisation's indirect emissions form part of their suppliers’ direct emissions and likely occur in other regions and jurisdictions, rendering them more abstract and intangible.</p><p>Quantifying indirect environmental impacts requires consideration of the supply chains delivering goods and services to final consumption. Supply chains link production layers together, where at each stage numerous inputs and components are combined to make intermediate products. This can be depicted as a tree branching upwards and outwards from the consumer, with each node representing a production stage (Box 1). Here, “upstream” refers to layers occurring before the product reaches a consumer, and “downstream” refers to layers after final consumption, including disposal of the product.</p><p>Environmental effects can occur at each layer and accumulate along the supply chain as more layers are included.<span><sup>6</sup></span> Eventually, supply chains reach consumers as final products. Accounting for all upstream environmental impacts associated with a product or service is onerous because of the large number of production layers and the many inputs into each layer. An illustrative example of supply chain is “fossil fuel combustion > petrochemical refining > plastic sample jars > pathology services”, which is just one of the many supply chains contributing to “pathology services”.<span><sup>7</sup></span></p><p>The “system boundary” is a conceptual limit within which environmental effects are captured by an assessment method.<span><sup>8</sup></span> The boundary is considered “incomplete” when all important activities are not within the boundary, resulting in some fraction of environmental effects being uncounted.<span><sup>9</sup></span> An awareness of the defined system boundary is important when calculating the full environmental footprint of a product or process and when making comparisons. The extent to which unaccounted impacts are significant depends on the process and activity and may include, for example, impacts arising from capital works, infrastructure and the services sector. Box 2 depicts the system boundary in relation to final consumption and intermediate production stages.</p><p>Although in common use, these scopes are a simplification and do not always neatly align with organisation structure or function. For example, emissions from ambulatory patient transport may be attributed to a health system's scope 1 emissions; however, patient self-transport emissions remain uncounted. In addition, the scope framework does not consider shared responsibility of emissions between upstream and downstream actors in the supply chain. These difficulties reflect wider societal complexities in attributing responsibility for emissions reductions.<span><sup>11</sup></span></p><p>Two main environmental footprinting methods can be distinguished: life cycle assessment (LCA) and environmentally extended input–output analysis (EE-IOA).</p><p>Which assessment technique should be used depends on the health care context and research question. In general, questions involving diagnostic methods and treatments are best answered using LCA techniques, whereas assessing overall progress at the health system level is more suited to EE-IOA. International Organization for Standardization (ISO) 14040:2006 and 14044:2006 provide guidelines to practitioners doing life cycle assessments. The European Union is introducing new regulations to combat greenwashing<span><sup>26</sup></span> and has its own guidelines on how LCAs should be done.<span><sup>27</sup></span> IOA and its extensions are also governed by global standards.<span><sup>28</sup></span> Adherence to these standards and guidelines can provide an indication of the quality and trustworthiness of sustainability assessments and enables comparison between studies.</p><p>Environmental impacts will increasingly need to be assessed and considered as part of health sector decision making at every level. However, systems for environmental data collection, storage and analysis are often limited in many health systems and usually not standardised or linked to clinical and population outcomes.<span><sup>29</sup></span> Information about product environmental performance is rarely provided by manufacturers, and the underlying data are often inaccessible.<span><sup>30</sup></span></p><p>Health care professionals have an important role in normalising consideration of the environmental impact of health care and advocating for availability of evidence and the supporting infrastructure to evaluate and reduce that impact. We are not suggesting that environmental footprinting is the primary role of health care workers, nor are we suggesting that considerations of environmental impact should take precedence over clinical outcomes. Rather, environmental sustainability should be considered as a dimension of quality, safety and good governance alongside patient and population health outcomes.</p><p>No relevant disclosures.</p><p>Not commissioned; externally peer reviewed.</p>\",\"PeriodicalId\":18214,\"journal\":{\"name\":\"Medical Journal of Australia\",\"volume\":\"221 9\",\"pages\":\"464-467\"},\"PeriodicalIF\":8.5000,\"publicationDate\":\"2024-10-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52481\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Journal of Australia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52481\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52481","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Environmental footprinting in health care: a primer
Health care systems are responsible for 4–5% of global greenhouse gas (GHG) emissions.1, 2 There is increasing pressure to reduce the environmental effects of health care as more health professionals recognise its contribution to climate change.3, 4 However, measuring environmental effects and assessing progress towards decarbonisation are not trivial processes because the mechanisms driving environmental burdens are often hidden. Although much of the early focus in health has been on decarbonisation of building and transport assets, most of health care's GHG emissions occur within the supply chains that provision the health care system before the final delivery of services.5
This article is intended to serve as a beginner's introduction to the environmental footprinting techniques that can be applied to uncover health care's environmental impacts, including impacts occurring along supply chains. This article focuses on GHG emissions, but many other pollutants and environmental stressors can be assessed using these methods.
Environmental impacts can be separated into “direct” and “indirect” impacts. Direct impacts occur within an organisation's physical boundary, for example hospital grounds. Indirect impacts occur outside this immediate boundary, for example impacts from purchased products. Direct impacts are relatively easy to estimate using fossil fuel consumption and utility bills. In contrast, estimating indirect emissions is more challenging for health care organisations and requires detailed data on the quantity or cost of procured products and services and the application of environmental footprinting techniques. An organisation's indirect emissions form part of their suppliers’ direct emissions and likely occur in other regions and jurisdictions, rendering them more abstract and intangible.
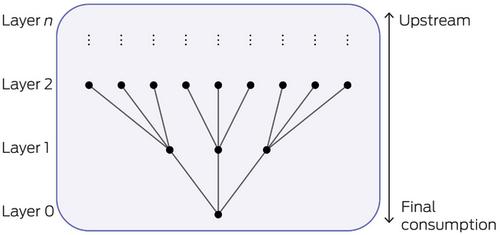
Quantifying indirect environmental impacts requires consideration of the supply chains delivering goods and services to final consumption. Supply chains link production layers together, where at each stage numerous inputs and components are combined to make intermediate products. This can be depicted as a tree branching upwards and outwards from the consumer, with each node representing a production stage (Box 1). Here, “upstream” refers to layers occurring before the product reaches a consumer, and “downstream” refers to layers after final consumption, including disposal of the product.
Environmental effects can occur at each layer and accumulate along the supply chain as more layers are included.6 Eventually, supply chains reach consumers as final products. Accounting for all upstream environmental impacts associated with a product or service is onerous because of the large number of production layers and the many inputs into each layer. An illustrative example of supply chain is “fossil fuel combustion > petrochemical refining > plastic sample jars > pathology services”, which is just one of the many supply chains contributing to “pathology services”.7
The “system boundary” is a conceptual limit within which environmental effects are captured by an assessment method.8 The boundary is considered “incomplete” when all important activities are not within the boundary, resulting in some fraction of environmental effects being uncounted.9 An awareness of the defined system boundary is important when calculating the full environmental footprint of a product or process and when making comparisons. The extent to which unaccounted impacts are significant depends on the process and activity and may include, for example, impacts arising from capital works, infrastructure and the services sector. Box 2 depicts the system boundary in relation to final consumption and intermediate production stages.
Although in common use, these scopes are a simplification and do not always neatly align with organisation structure or function. For example, emissions from ambulatory patient transport may be attributed to a health system's scope 1 emissions; however, patient self-transport emissions remain uncounted. In addition, the scope framework does not consider shared responsibility of emissions between upstream and downstream actors in the supply chain. These difficulties reflect wider societal complexities in attributing responsibility for emissions reductions.11
Two main environmental footprinting methods can be distinguished: life cycle assessment (LCA) and environmentally extended input–output analysis (EE-IOA).
Which assessment technique should be used depends on the health care context and research question. In general, questions involving diagnostic methods and treatments are best answered using LCA techniques, whereas assessing overall progress at the health system level is more suited to EE-IOA. International Organization for Standardization (ISO) 14040:2006 and 14044:2006 provide guidelines to practitioners doing life cycle assessments. The European Union is introducing new regulations to combat greenwashing26 and has its own guidelines on how LCAs should be done.27 IOA and its extensions are also governed by global standards.28 Adherence to these standards and guidelines can provide an indication of the quality and trustworthiness of sustainability assessments and enables comparison between studies.
Environmental impacts will increasingly need to be assessed and considered as part of health sector decision making at every level. However, systems for environmental data collection, storage and analysis are often limited in many health systems and usually not standardised or linked to clinical and population outcomes.29 Information about product environmental performance is rarely provided by manufacturers, and the underlying data are often inaccessible.30
Health care professionals have an important role in normalising consideration of the environmental impact of health care and advocating for availability of evidence and the supporting infrastructure to evaluate and reduce that impact. We are not suggesting that environmental footprinting is the primary role of health care workers, nor are we suggesting that considerations of environmental impact should take precedence over clinical outcomes. Rather, environmental sustainability should be considered as a dimension of quality, safety and good governance alongside patient and population health outcomes.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
