Catherine B Jensen, Elizabeth M Bacon, Lauren N Krumeich, Hunter J Underwood, David T Hughes, Paul G Gauger, Richard Burney, Susan C Pitt
{"title":"为甲状腺癌手术制定大规模质量改进计划。","authors":"Catherine B Jensen, Elizabeth M Bacon, Lauren N Krumeich, Hunter J Underwood, David T Hughes, Paul G Gauger, Richard Burney, Susan C Pitt","doi":"10.1002/wjs.12367","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical quality improvement (QI) plays a critical role in optimizing patient outcomes and reducing healthcare costs. QI programs focusing specifically on thyroid cancer surgical care are lacking. This study aimed to (a) select and introduce surgical quality indicators for thyroid cancer and (b) identify areas for QI at the state-level.</p><p><strong>Methods: </strong>A multidisciplinary team of thyroid cancer and QI experts selected 10 thyroid cancer-specific quality indicators and assessed the quality of thyroid cancer surgical care compared to current national guidelines. Analysis of the first year (January-December 2023) of data collection was performed using descriptive statistics.</p><p><strong>Results: </strong>The thyroid cancer quality indicators included preoperative cytology, postoperative pathology, staging, cancer size, margin status, extrathyroidal extension, lymph nodes, postoperative complications within 30 days, documented follow-up treatment, and documented surveillance plans. 112 surgeons performed 360 thyroidectomies for thyroid cancer at 51 hospitals. Preoperative cytology was not performed in 34.3% (n = 103) of cases with thyroid cancer on final pathology. When the extent of surgery was evaluated by papillary cancer size, 50.0% (n = 38) of patients with <1 cm cancers underwent total thyroidectomy, and 13.8% (n = 4) with >4 cm underwent thyroid lobectomy. Positive margins were found in 16.2% (n = 53). Postoperatively, 19.2% (n = 69) of patients lacked documented follow-up, and 18.6% (n = 67) lacked thyroid cancer surveillance plans.</p><p><strong>Conclusions: </strong>Establishing a dedicated QI program for thyroid cancer provides a previously unharnessed opportunity to enhance the quality of thyroid cancer surgical care. Statewide surgical quality collaboratives offer a model for establishing thyroid cancer QI initiatives across diverse healthcare settings in other states and countries.</p>","PeriodicalId":23926,"journal":{"name":"World Journal of Surgery","volume":" ","pages":"2925-2933"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11619744/pdf/","citationCount":"0","resultStr":"{\"title\":\"Developing a large-scale quality improvement program for thyroid cancer surgery.\",\"authors\":\"Catherine B Jensen, Elizabeth M Bacon, Lauren N Krumeich, Hunter J Underwood, David T Hughes, Paul G Gauger, Richard Burney, Susan C Pitt\",\"doi\":\"10.1002/wjs.12367\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Surgical quality improvement (QI) plays a critical role in optimizing patient outcomes and reducing healthcare costs. QI programs focusing specifically on thyroid cancer surgical care are lacking. This study aimed to (a) select and introduce surgical quality indicators for thyroid cancer and (b) identify areas for QI at the state-level.</p><p><strong>Methods: </strong>A multidisciplinary team of thyroid cancer and QI experts selected 10 thyroid cancer-specific quality indicators and assessed the quality of thyroid cancer surgical care compared to current national guidelines. Analysis of the first year (January-December 2023) of data collection was performed using descriptive statistics.</p><p><strong>Results: </strong>The thyroid cancer quality indicators included preoperative cytology, postoperative pathology, staging, cancer size, margin status, extrathyroidal extension, lymph nodes, postoperative complications within 30 days, documented follow-up treatment, and documented surveillance plans. 112 surgeons performed 360 thyroidectomies for thyroid cancer at 51 hospitals. Preoperative cytology was not performed in 34.3% (n = 103) of cases with thyroid cancer on final pathology. When the extent of surgery was evaluated by papillary cancer size, 50.0% (n = 38) of patients with <1 cm cancers underwent total thyroidectomy, and 13.8% (n = 4) with >4 cm underwent thyroid lobectomy. Positive margins were found in 16.2% (n = 53). Postoperatively, 19.2% (n = 69) of patients lacked documented follow-up, and 18.6% (n = 67) lacked thyroid cancer surveillance plans.</p><p><strong>Conclusions: </strong>Establishing a dedicated QI program for thyroid cancer provides a previously unharnessed opportunity to enhance the quality of thyroid cancer surgical care. Statewide surgical quality collaboratives offer a model for establishing thyroid cancer QI initiatives across diverse healthcare settings in other states and countries.</p>\",\"PeriodicalId\":23926,\"journal\":{\"name\":\"World Journal of Surgery\",\"volume\":\" \",\"pages\":\"2925-2933\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11619744/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/wjs.12367\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/wjs.12367","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Developing a large-scale quality improvement program for thyroid cancer surgery.
Background: Surgical quality improvement (QI) plays a critical role in optimizing patient outcomes and reducing healthcare costs. QI programs focusing specifically on thyroid cancer surgical care are lacking. This study aimed to (a) select and introduce surgical quality indicators for thyroid cancer and (b) identify areas for QI at the state-level.
Methods: A multidisciplinary team of thyroid cancer and QI experts selected 10 thyroid cancer-specific quality indicators and assessed the quality of thyroid cancer surgical care compared to current national guidelines. Analysis of the first year (January-December 2023) of data collection was performed using descriptive statistics.
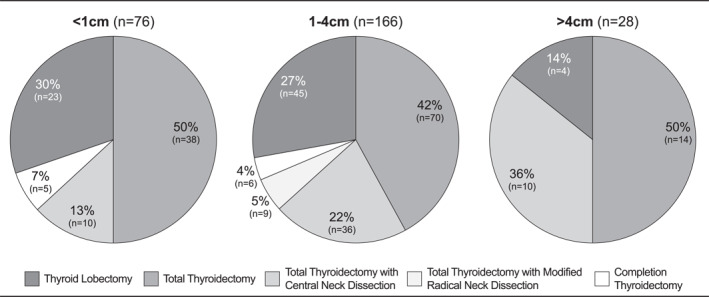
Results: The thyroid cancer quality indicators included preoperative cytology, postoperative pathology, staging, cancer size, margin status, extrathyroidal extension, lymph nodes, postoperative complications within 30 days, documented follow-up treatment, and documented surveillance plans. 112 surgeons performed 360 thyroidectomies for thyroid cancer at 51 hospitals. Preoperative cytology was not performed in 34.3% (n = 103) of cases with thyroid cancer on final pathology. When the extent of surgery was evaluated by papillary cancer size, 50.0% (n = 38) of patients with <1 cm cancers underwent total thyroidectomy, and 13.8% (n = 4) with >4 cm underwent thyroid lobectomy. Positive margins were found in 16.2% (n = 53). Postoperatively, 19.2% (n = 69) of patients lacked documented follow-up, and 18.6% (n = 67) lacked thyroid cancer surveillance plans.
Conclusions: Establishing a dedicated QI program for thyroid cancer provides a previously unharnessed opportunity to enhance the quality of thyroid cancer surgical care. Statewide surgical quality collaboratives offer a model for establishing thyroid cancer QI initiatives across diverse healthcare settings in other states and countries.
期刊介绍:
World Journal of Surgery is the official publication of the International Society of Surgery/Societe Internationale de Chirurgie (iss-sic.com). Under the editorship of Dr. Julie Ann Sosa, World Journal of Surgery provides an in-depth, international forum for the most authoritative information on major clinical problems in the fields of clinical and experimental surgery, surgical education, and socioeconomic aspects of surgical care. Contributions are reviewed and selected by a group of distinguished surgeons from across the world who make up the Editorial Board.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
