{"title":"癫痫手术中的清醒开颅术:病例系列和三种不同情况的建议。","authors":"Takehiro Uda, Yuta Tanoue, Toshiyuki Kawashima, Vich Yindeedej, Shugo Nishijima, Noritsugu Kunihiro, Ryoko Umaba, Kotaro Ishimoto, Takeo Goto","doi":"10.3390/brainsci14100958","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Awake craniotomy (AWC) allows intraoperative evaluation of functions involving the cortical surface and subcortical fibers. In epilepsy surgery, indications for and the role of AWC have not been established because evaluation with intracranial electrodes is considered the gold standard. We report herein our case series of patients who underwent AWC in epilepsy surgery and propose the scenarios for and roles of AWC.</p><p><strong>Methods: </strong>Patients who underwent AWC in epilepsy surgery at our institutions between 2014 and 2023 were included. Information about age, sex, etiology, location of epileptogenicity, seizure type, use of intracranial electrode placement, surgical complications, neurological deficits, additional surgery, and seizure outcomes was reviewed. Following a diagnostic and treatment flow for epilepsy surgery, we clarified three different scenarios and roles for AWC.</p><p><strong>Results: </strong>Ten patients underwent AWC. Three patients underwent AWC after non-invasive evaluations. Two patients underwent AWC after intracranial evaluation with stereotactic electroencephalography (SEEG). Five patients underwent AWC after intracranial evaluation with subdural grid electrodes (SDG). Among these, two patients were initially evaluated with SEEG and with SDG thereafter. One patient reported slight numbness in the hand, and one patient showed slight cognitive decline. Seizure outcomes according to the Engel outcome scale were class 1A in three patients, IIA in two patients, IIIA in four patients, and IVA in one patient.</p><p><strong>Conclusions: </strong>AWC can be used for purposes of epilepsy surgery in different situations, either immediately after non-invasive studies or as an additional invasive step after invasive monitoring with either SEEG or SDG. The application of AWC should be individualized according to each patient's specific characteristics.</p>","PeriodicalId":9095,"journal":{"name":"Brain Sciences","volume":"14 10","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506450/pdf/","citationCount":"0","resultStr":"{\"title\":\"Awake Craniotomy in Epilepsy Surgery: A Case Series and Proposal for Three Different Scenarios.\",\"authors\":\"Takehiro Uda, Yuta Tanoue, Toshiyuki Kawashima, Vich Yindeedej, Shugo Nishijima, Noritsugu Kunihiro, Ryoko Umaba, Kotaro Ishimoto, Takeo Goto\",\"doi\":\"10.3390/brainsci14100958\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Awake craniotomy (AWC) allows intraoperative evaluation of functions involving the cortical surface and subcortical fibers. In epilepsy surgery, indications for and the role of AWC have not been established because evaluation with intracranial electrodes is considered the gold standard. We report herein our case series of patients who underwent AWC in epilepsy surgery and propose the scenarios for and roles of AWC.</p><p><strong>Methods: </strong>Patients who underwent AWC in epilepsy surgery at our institutions between 2014 and 2023 were included. Information about age, sex, etiology, location of epileptogenicity, seizure type, use of intracranial electrode placement, surgical complications, neurological deficits, additional surgery, and seizure outcomes was reviewed. Following a diagnostic and treatment flow for epilepsy surgery, we clarified three different scenarios and roles for AWC.</p><p><strong>Results: </strong>Ten patients underwent AWC. Three patients underwent AWC after non-invasive evaluations. Two patients underwent AWC after intracranial evaluation with stereotactic electroencephalography (SEEG). Five patients underwent AWC after intracranial evaluation with subdural grid electrodes (SDG). Among these, two patients were initially evaluated with SEEG and with SDG thereafter. One patient reported slight numbness in the hand, and one patient showed slight cognitive decline. Seizure outcomes according to the Engel outcome scale were class 1A in three patients, IIA in two patients, IIIA in four patients, and IVA in one patient.</p><p><strong>Conclusions: </strong>AWC can be used for purposes of epilepsy surgery in different situations, either immediately after non-invasive studies or as an additional invasive step after invasive monitoring with either SEEG or SDG. The application of AWC should be individualized according to each patient's specific characteristics.</p>\",\"PeriodicalId\":9095,\"journal\":{\"name\":\"Brain Sciences\",\"volume\":\"14 10\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506450/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain Sciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/brainsci14100958\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/brainsci14100958","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
Awake Craniotomy in Epilepsy Surgery: A Case Series and Proposal for Three Different Scenarios.
Objective: Awake craniotomy (AWC) allows intraoperative evaluation of functions involving the cortical surface and subcortical fibers. In epilepsy surgery, indications for and the role of AWC have not been established because evaluation with intracranial electrodes is considered the gold standard. We report herein our case series of patients who underwent AWC in epilepsy surgery and propose the scenarios for and roles of AWC.
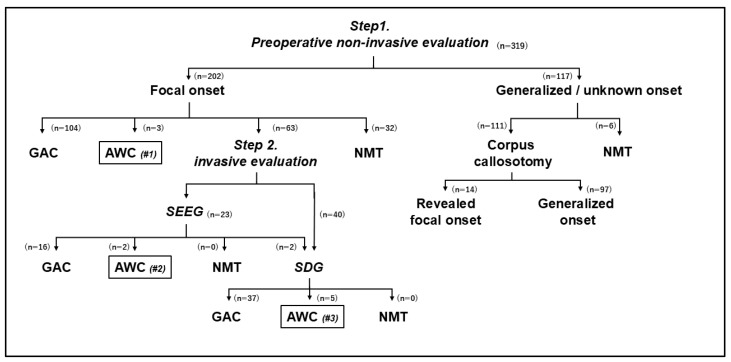
Methods: Patients who underwent AWC in epilepsy surgery at our institutions between 2014 and 2023 were included. Information about age, sex, etiology, location of epileptogenicity, seizure type, use of intracranial electrode placement, surgical complications, neurological deficits, additional surgery, and seizure outcomes was reviewed. Following a diagnostic and treatment flow for epilepsy surgery, we clarified three different scenarios and roles for AWC.
Results: Ten patients underwent AWC. Three patients underwent AWC after non-invasive evaluations. Two patients underwent AWC after intracranial evaluation with stereotactic electroencephalography (SEEG). Five patients underwent AWC after intracranial evaluation with subdural grid electrodes (SDG). Among these, two patients were initially evaluated with SEEG and with SDG thereafter. One patient reported slight numbness in the hand, and one patient showed slight cognitive decline. Seizure outcomes according to the Engel outcome scale were class 1A in three patients, IIA in two patients, IIIA in four patients, and IVA in one patient.
Conclusions: AWC can be used for purposes of epilepsy surgery in different situations, either immediately after non-invasive studies or as an additional invasive step after invasive monitoring with either SEEG or SDG. The application of AWC should be individualized according to each patient's specific characteristics.
期刊介绍:
Brain Sciences (ISSN 2076-3425) is a peer-reviewed scientific journal that publishes original articles, critical reviews, research notes and short communications in the areas of cognitive neuroscience, developmental neuroscience, molecular and cellular neuroscience, neural engineering, neuroimaging, neurolinguistics, neuropathy, systems neuroscience, and theoretical and computational neuroscience. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. There is no restriction on the length of the papers. The full experimental details must be provided so that the results can be reproduced. Electronic files or software regarding the full details of the calculation and experimental procedure, if unable to be published in a normal way, can be deposited as supplementary material.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
