Valentina Barletta, Antonio Maria Canu, Matteo Parollo, Andrea Di Cori, Luca Segreti, Raffaele De Lucia, Maria Grazia Bongiorni, Giulio Zucchelli
{"title":"导管消融术后心房机电间隔长与心律失常复发有关:如何找回失去的东西?","authors":"Valentina Barletta, Antonio Maria Canu, Matteo Parollo, Andrea Di Cori, Luca Segreti, Raffaele De Lucia, Maria Grazia Bongiorni, Giulio Zucchelli","doi":"10.4103/jcecho.jcecho_35_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) results in electrical and structural remodeling of the atria, which extent is known to be associated with a higher AF recurrence rate after catheter ablation (CA). Recently, a novel echocardiographic parameter derived from tissue Doppler imaging (TDI) [PA-TDI] has been introduced to assess the total atrial activation time, as a noninvasive surrogate of fibrosis and remodeling. The aim of the study is to investigate the role of PA-TDI interval as a predictor of AF ablation efficacy.</p><p><strong>Methods: </strong>We retrospectively included patients with paroxysmal symptomatic drug-refractory AF referred to our institution for CA procedure, who presented sinus rhythm at admission. A complete transthoracic echocardiogram was performed before the ablation procedure, including the assessment of PA-TDI interval.</p><p><strong>Results: </strong>From January 2015 to April 2018, 128 patients (mean age: 61.86 ± 9.08 years, 68% male, body surface area: 1.97 ± 0.21 mq, body mass index: 26.98 ± 3.86 kg/mq, and ejection fraction: 59% ±6.06%) with symptomatic drug-refractory AF who received radiofrequency CA were enrolled. During the follow-up of 15.80 ± 6.7 months, 30 patients (23%) developed AF recurrence out of the blanking period. Compared with those without recurrence (group 1), patients with recurrence (group 2) had a larger left atrium (LA) size (Group 1 vs. Group 2: mean LA area: 22.2 ± 4.6 cmq vs. 25 ± 6.6 cmq, <i>P</i> = 0.015; mean indexed LA volume: 35 ± 10 mL/mq vs. 40 ± 12 mL/mq, <i>P</i> = 0.04) and longer PA-TDI interval (Group 1 vs. Group 2: 162 ± 33 ms vs. 133 ± 26 ms, <i>P</i> < 0.0001). A cutoff of PA-TDI > 150 ms identified patients with recurrence after ablation with a sensibility of 82% and specificity of 83% (area under the curve 0.879).</p><p><strong>Conclusions: </strong>The total activation time assessed by PA-TDI is an independent predictor of AF recurrence and can be used to predict the efficacy of transcatheter ablation.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"34 3","pages":"125-131"},"PeriodicalIF":1.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11495311/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Long Atrial Electromechanical Interval is Associated with Arrhythmic Recurrence after Catheter Ablation: How to Find What Has Been Lost.\",\"authors\":\"Valentina Barletta, Antonio Maria Canu, Matteo Parollo, Andrea Di Cori, Luca Segreti, Raffaele De Lucia, Maria Grazia Bongiorni, Giulio Zucchelli\",\"doi\":\"10.4103/jcecho.jcecho_35_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Atrial fibrillation (AF) results in electrical and structural remodeling of the atria, which extent is known to be associated with a higher AF recurrence rate after catheter ablation (CA). Recently, a novel echocardiographic parameter derived from tissue Doppler imaging (TDI) [PA-TDI] has been introduced to assess the total atrial activation time, as a noninvasive surrogate of fibrosis and remodeling. The aim of the study is to investigate the role of PA-TDI interval as a predictor of AF ablation efficacy.</p><p><strong>Methods: </strong>We retrospectively included patients with paroxysmal symptomatic drug-refractory AF referred to our institution for CA procedure, who presented sinus rhythm at admission. A complete transthoracic echocardiogram was performed before the ablation procedure, including the assessment of PA-TDI interval.</p><p><strong>Results: </strong>From January 2015 to April 2018, 128 patients (mean age: 61.86 ± 9.08 years, 68% male, body surface area: 1.97 ± 0.21 mq, body mass index: 26.98 ± 3.86 kg/mq, and ejection fraction: 59% ±6.06%) with symptomatic drug-refractory AF who received radiofrequency CA were enrolled. During the follow-up of 15.80 ± 6.7 months, 30 patients (23%) developed AF recurrence out of the blanking period. Compared with those without recurrence (group 1), patients with recurrence (group 2) had a larger left atrium (LA) size (Group 1 vs. Group 2: mean LA area: 22.2 ± 4.6 cmq vs. 25 ± 6.6 cmq, <i>P</i> = 0.015; mean indexed LA volume: 35 ± 10 mL/mq vs. 40 ± 12 mL/mq, <i>P</i> = 0.04) and longer PA-TDI interval (Group 1 vs. Group 2: 162 ± 33 ms vs. 133 ± 26 ms, <i>P</i> < 0.0001). A cutoff of PA-TDI > 150 ms identified patients with recurrence after ablation with a sensibility of 82% and specificity of 83% (area under the curve 0.879).</p><p><strong>Conclusions: </strong>The total activation time assessed by PA-TDI is an independent predictor of AF recurrence and can be used to predict the efficacy of transcatheter ablation.</p>\",\"PeriodicalId\":15191,\"journal\":{\"name\":\"Journal of Cardiovascular Echography\",\"volume\":\"34 3\",\"pages\":\"125-131\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11495311/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Echography\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcecho.jcecho_35_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_35_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A Long Atrial Electromechanical Interval is Associated with Arrhythmic Recurrence after Catheter Ablation: How to Find What Has Been Lost.
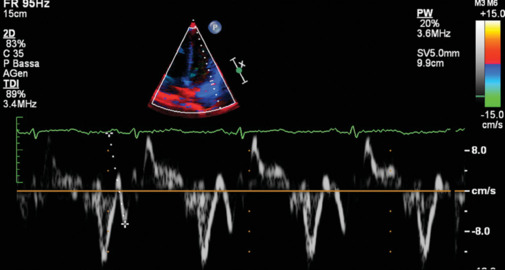
Background: Atrial fibrillation (AF) results in electrical and structural remodeling of the atria, which extent is known to be associated with a higher AF recurrence rate after catheter ablation (CA). Recently, a novel echocardiographic parameter derived from tissue Doppler imaging (TDI) [PA-TDI] has been introduced to assess the total atrial activation time, as a noninvasive surrogate of fibrosis and remodeling. The aim of the study is to investigate the role of PA-TDI interval as a predictor of AF ablation efficacy.
Methods: We retrospectively included patients with paroxysmal symptomatic drug-refractory AF referred to our institution for CA procedure, who presented sinus rhythm at admission. A complete transthoracic echocardiogram was performed before the ablation procedure, including the assessment of PA-TDI interval.
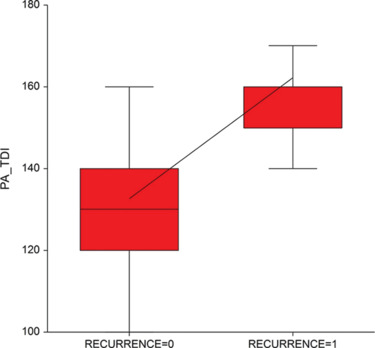
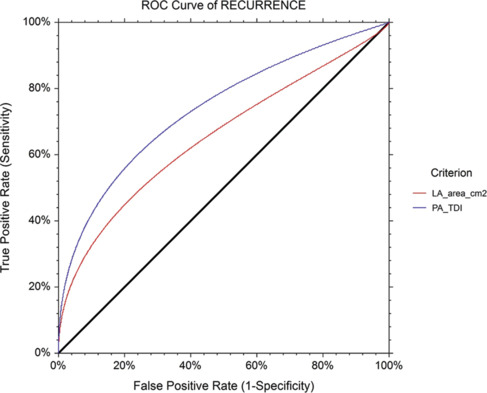
Results: From January 2015 to April 2018, 128 patients (mean age: 61.86 ± 9.08 years, 68% male, body surface area: 1.97 ± 0.21 mq, body mass index: 26.98 ± 3.86 kg/mq, and ejection fraction: 59% ±6.06%) with symptomatic drug-refractory AF who received radiofrequency CA were enrolled. During the follow-up of 15.80 ± 6.7 months, 30 patients (23%) developed AF recurrence out of the blanking period. Compared with those without recurrence (group 1), patients with recurrence (group 2) had a larger left atrium (LA) size (Group 1 vs. Group 2: mean LA area: 22.2 ± 4.6 cmq vs. 25 ± 6.6 cmq, P = 0.015; mean indexed LA volume: 35 ± 10 mL/mq vs. 40 ± 12 mL/mq, P = 0.04) and longer PA-TDI interval (Group 1 vs. Group 2: 162 ± 33 ms vs. 133 ± 26 ms, P < 0.0001). A cutoff of PA-TDI > 150 ms identified patients with recurrence after ablation with a sensibility of 82% and specificity of 83% (area under the curve 0.879).
Conclusions: The total activation time assessed by PA-TDI is an independent predictor of AF recurrence and can be used to predict the efficacy of transcatheter ablation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
