Vasudeva G Iyer, Lisa B E Shields, Michael W Daniels, Yi Ping Zhang, Christopher B Shields
{"title":"肘前外侧皮肤神经病的回顾性研究:49 例病例的电诊断结果和病因。","authors":"Vasudeva G Iyer, Lisa B E Shields, Michael W Daniels, Yi Ping Zhang, Christopher B Shields","doi":"10.3390/neurolint16050086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The lateral antebrachial cutaneous nerve (LACN) is the terminal sensory branch of the musculocutaneous nerve and is rarely entrapped or injured. This study describes the electrodiagnostic (EDX) findings and etiologies of LACN neuropathy.</p><p><strong>Methods: </strong>This is a review of 49 patients with pain and/or paresthesia of the forearm who underwent EDX studies. The diagnosis of LACN neuropathy was based on clinical and sensory conduction abnormalities.</p><p><strong>Results: </strong>The most common etiology of LACN neuropathy was iatrogenic injury in 30 (61.2%) patients, primarily due to biceps tendon repair at the elbow (11 [36.7%]) and phlebotomy (5 [16.7%]). Fifteen (30.6%) patients sustained a non-iatrogenic injury at the proximal forearm/elbow, consisting of six (60%) laceration injuries and five (33.3%) stretch injuries. Four (8.2%) patients comprised the \"other\" etiology category, including two mass lesions causing LACN compression. Pain, paresthesia, and/or numbness in the LACN distribution were reported in 33 (67.3%), 27 (55.1%), and 23 (46.9%) patients, respectively. Hypoesthesia was detected in 45 (91.8%) patients, and dysesthesia in 7 (14.3%). The sensory nerve action potentials (SNAPs) of the LACN on the symptomatic side were absent in 44 (89.8%) patients. Of the five patients whose SNAPs of the LACN were detected, all had a decreased amplitude, and two had increased sensory latency.</p><p><strong>Conclusions: </strong>The most common etiology for LACN neuropathy in this series was iatrogenic injury; repair of biceps tendon at the elbow was the most frequent provoking cause. Protection of the LACN during surgical procedures at the elbow and forearm is vital to prevent iatrogenic injury.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"16 5","pages":"1143-1157"},"PeriodicalIF":3.0000,"publicationDate":"2024-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11510289/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Retrospective Study of Lateral Antebrachial Cutaneous Nerve Neuropathy: Electrodiagnostic Findings and Etiologies in 49 Cases.\",\"authors\":\"Vasudeva G Iyer, Lisa B E Shields, Michael W Daniels, Yi Ping Zhang, Christopher B Shields\",\"doi\":\"10.3390/neurolint16050086\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The lateral antebrachial cutaneous nerve (LACN) is the terminal sensory branch of the musculocutaneous nerve and is rarely entrapped or injured. This study describes the electrodiagnostic (EDX) findings and etiologies of LACN neuropathy.</p><p><strong>Methods: </strong>This is a review of 49 patients with pain and/or paresthesia of the forearm who underwent EDX studies. The diagnosis of LACN neuropathy was based on clinical and sensory conduction abnormalities.</p><p><strong>Results: </strong>The most common etiology of LACN neuropathy was iatrogenic injury in 30 (61.2%) patients, primarily due to biceps tendon repair at the elbow (11 [36.7%]) and phlebotomy (5 [16.7%]). Fifteen (30.6%) patients sustained a non-iatrogenic injury at the proximal forearm/elbow, consisting of six (60%) laceration injuries and five (33.3%) stretch injuries. Four (8.2%) patients comprised the \\\"other\\\" etiology category, including two mass lesions causing LACN compression. Pain, paresthesia, and/or numbness in the LACN distribution were reported in 33 (67.3%), 27 (55.1%), and 23 (46.9%) patients, respectively. Hypoesthesia was detected in 45 (91.8%) patients, and dysesthesia in 7 (14.3%). The sensory nerve action potentials (SNAPs) of the LACN on the symptomatic side were absent in 44 (89.8%) patients. Of the five patients whose SNAPs of the LACN were detected, all had a decreased amplitude, and two had increased sensory latency.</p><p><strong>Conclusions: </strong>The most common etiology for LACN neuropathy in this series was iatrogenic injury; repair of biceps tendon at the elbow was the most frequent provoking cause. Protection of the LACN during surgical procedures at the elbow and forearm is vital to prevent iatrogenic injury.</p>\",\"PeriodicalId\":19130,\"journal\":{\"name\":\"Neurology International\",\"volume\":\"16 5\",\"pages\":\"1143-1157\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2024-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11510289/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/neurolint16050086\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint16050086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
A Retrospective Study of Lateral Antebrachial Cutaneous Nerve Neuropathy: Electrodiagnostic Findings and Etiologies in 49 Cases.
Background: The lateral antebrachial cutaneous nerve (LACN) is the terminal sensory branch of the musculocutaneous nerve and is rarely entrapped or injured. This study describes the electrodiagnostic (EDX) findings and etiologies of LACN neuropathy.
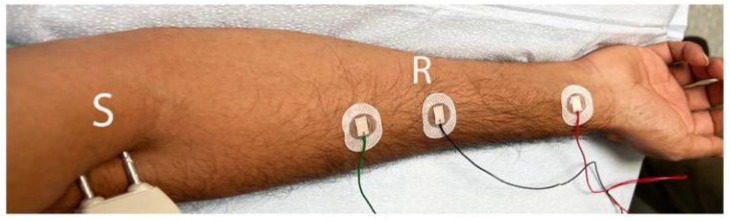
Methods: This is a review of 49 patients with pain and/or paresthesia of the forearm who underwent EDX studies. The diagnosis of LACN neuropathy was based on clinical and sensory conduction abnormalities.
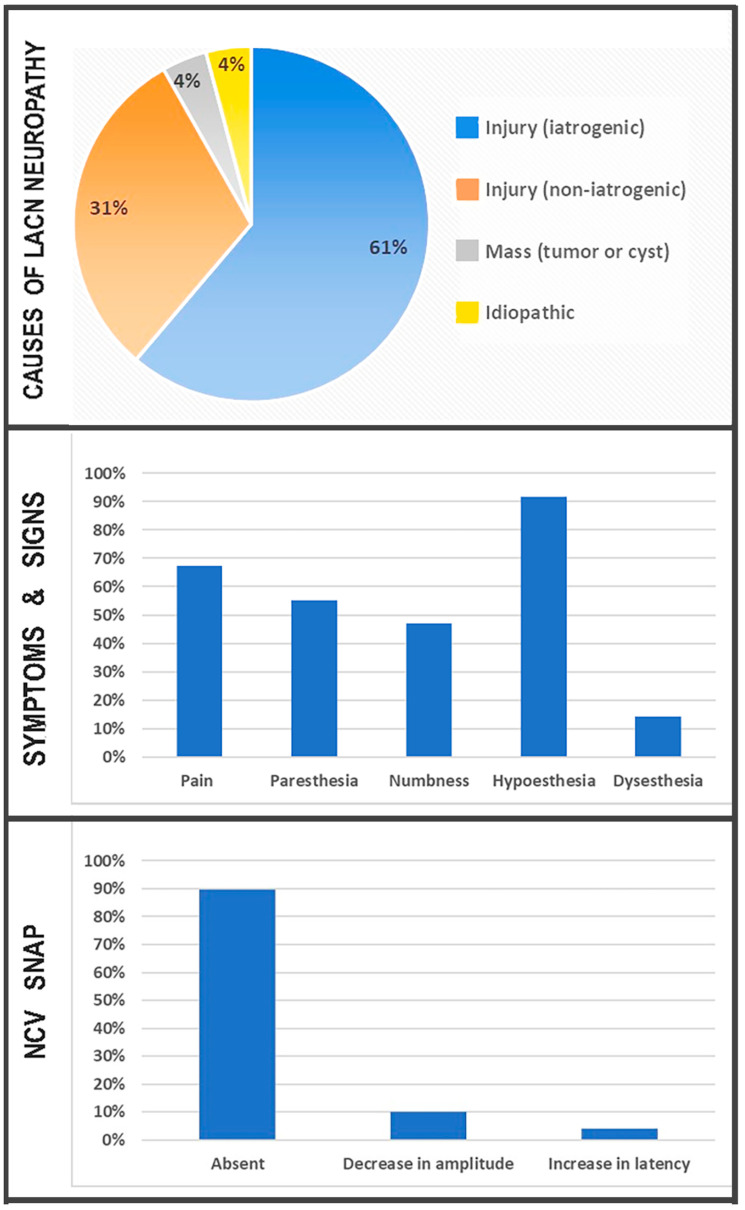
Results: The most common etiology of LACN neuropathy was iatrogenic injury in 30 (61.2%) patients, primarily due to biceps tendon repair at the elbow (11 [36.7%]) and phlebotomy (5 [16.7%]). Fifteen (30.6%) patients sustained a non-iatrogenic injury at the proximal forearm/elbow, consisting of six (60%) laceration injuries and five (33.3%) stretch injuries. Four (8.2%) patients comprised the "other" etiology category, including two mass lesions causing LACN compression. Pain, paresthesia, and/or numbness in the LACN distribution were reported in 33 (67.3%), 27 (55.1%), and 23 (46.9%) patients, respectively. Hypoesthesia was detected in 45 (91.8%) patients, and dysesthesia in 7 (14.3%). The sensory nerve action potentials (SNAPs) of the LACN on the symptomatic side were absent in 44 (89.8%) patients. Of the five patients whose SNAPs of the LACN were detected, all had a decreased amplitude, and two had increased sensory latency.
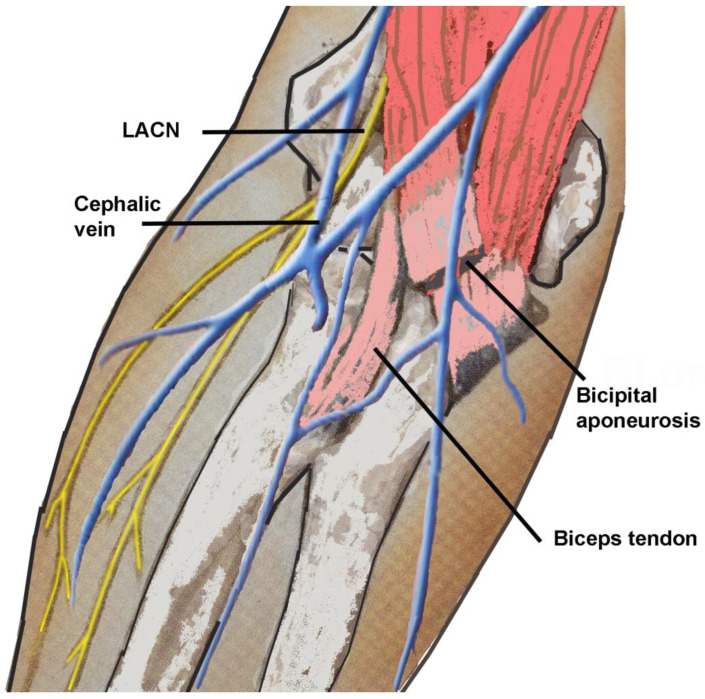
Conclusions: The most common etiology for LACN neuropathy in this series was iatrogenic injury; repair of biceps tendon at the elbow was the most frequent provoking cause. Protection of the LACN during surgical procedures at the elbow and forearm is vital to prevent iatrogenic injury.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
