Tanja Sprave, Raluca Stoian, Natalia Volegova-Neher, Mark Gainey, Michael Kollefrath, Dimos Baltas, Anca-Ligia Grosu, Ingolf Juhasz-Böss, Rieke Schröder, Florin-Andrei Taran
{"title":"结合根治性手术和术中放疗的多模式方法在治疗妇科恶性肿瘤复发中的价值--对一家三级医疗中心大型患者队列的分析。","authors":"Tanja Sprave, Raluca Stoian, Natalia Volegova-Neher, Mark Gainey, Michael Kollefrath, Dimos Baltas, Anca-Ligia Grosu, Ingolf Juhasz-Böss, Rieke Schröder, Florin-Andrei Taran","doi":"10.1186/s13014-024-02537-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recurrent and locally advanced gynecological malignancies have a poor prognosis. In particularly, pelvic local recurrence after previous radiotherapy and/or positive resection margins during surgical treatment for recurrent disease result in low survival rates. Consequently, locoregional control is of utmost importance in this cohort of patients. The aim of this study was to analyze treatment outcomes and determine prognostic factors for patients treated with surgery and intraoperative radiotherapy (IORT) for recurrent and locally advanced gynecological malignancies.</p><p><strong>Methods: </strong>40 patients who underwent surgical treatment and IORT between 2010 and 2022 were eligible for inclusion. The median follow-up time was 22 months. The outcomes measured were locoregional control (LRC), overall survival (OS), and survival without distant metastases (DMFS). The Cox proportional hazards model was used for univariate and multivariate analysis to assess the impact of patient variables and treatment factors on the endpoints mentioned. The following variables were analyzed: age at surgical treatment and IORT and initial diagnosis (< 65 vs. ≥65 years, each), disease-free interval (DFI) between initial diagnosis and first recurrence, DFI to surgical treatment and IORT, grading, histology, IORT dose (≤ 13 vs. >13 Gy) and technique (high dose radiotherapy (HDR) vs. IORT using electrons, (IOERT)). Survival curves were generated using the Kaplan-Meier method.</p><p><strong>Results: </strong>The mean IORT dose was 13.8 Gy (range 10-18 Gy). Cervical carcinoma was most frequently found in 27.5% of patients followed by endometrial carcinoma and vulvar carcinoma in 25% respectively. The final histopathologic results after surgery with IORT showed no residual tumour in 24 patients (60%), microscopic residual disease in 5 patients (12.5%), resection status could not be evaluated in three patients (7.5%) and the resection status was unknown in eight patients (20%). Subsequently, 27.5% of patients also received adjuvant radiotherapy of the local recurrence bed. However, after IORT, 65% of the women suffered a recurrence. Of these, the recurrences were localized: in-field 32.5%, out-of-field 22.5% and margin-of-field 12.5%. The 3- and 5-year OS was 69% and 55% respectively. The 3- and 5-year LRC was 56% respectively. The 3- and 5-year DMFS was 66% and 49%. Whereas the comparison between groups by IORT dose level (≤ 13 vs. >13 Gy) showed a non-significant trend in favor of the higher dose only for OS (p = 0.094), but not in LRC and DMFS (p > 0.05). OS and DMFS, but not LRC, differed significantly between the HDR-IORT and IOERT groups (p = 0.06 and p = 0.03,) in favor of the HDR-IORT technique. For HDR-IORT technique a trend towards superior OS and LRC was observed in the univariate analysis: HR 3.76, CI 95%: 0.95-14.881, p = 0.059 and HR 2.165 CI 95%: 0.916-5.114, p = 0.078 CONCLUSIONS: The survival rate for pelvic recurrence in gynecological malignancies remains poor and comparable with historical data from the last two decades. Particularly HDR-IORT, appears to provide a long-term oncological benefit in carefully selected patients.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"19 1","pages":"147"},"PeriodicalIF":3.3000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515090/pdf/","citationCount":"0","resultStr":"{\"title\":\"The value of a multimodal approach combining radical surgery and intraoperative radiotherapy in the recurrence treatment of gynecological malignancies - analysis of a large patient cohort in a tertiary care center.\",\"authors\":\"Tanja Sprave, Raluca Stoian, Natalia Volegova-Neher, Mark Gainey, Michael Kollefrath, Dimos Baltas, Anca-Ligia Grosu, Ingolf Juhasz-Böss, Rieke Schröder, Florin-Andrei Taran\",\"doi\":\"10.1186/s13014-024-02537-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Recurrent and locally advanced gynecological malignancies have a poor prognosis. In particularly, pelvic local recurrence after previous radiotherapy and/or positive resection margins during surgical treatment for recurrent disease result in low survival rates. Consequently, locoregional control is of utmost importance in this cohort of patients. The aim of this study was to analyze treatment outcomes and determine prognostic factors for patients treated with surgery and intraoperative radiotherapy (IORT) for recurrent and locally advanced gynecological malignancies.</p><p><strong>Methods: </strong>40 patients who underwent surgical treatment and IORT between 2010 and 2022 were eligible for inclusion. The median follow-up time was 22 months. The outcomes measured were locoregional control (LRC), overall survival (OS), and survival without distant metastases (DMFS). The Cox proportional hazards model was used for univariate and multivariate analysis to assess the impact of patient variables and treatment factors on the endpoints mentioned. The following variables were analyzed: age at surgical treatment and IORT and initial diagnosis (< 65 vs. ≥65 years, each), disease-free interval (DFI) between initial diagnosis and first recurrence, DFI to surgical treatment and IORT, grading, histology, IORT dose (≤ 13 vs. >13 Gy) and technique (high dose radiotherapy (HDR) vs. IORT using electrons, (IOERT)). Survival curves were generated using the Kaplan-Meier method.</p><p><strong>Results: </strong>The mean IORT dose was 13.8 Gy (range 10-18 Gy). Cervical carcinoma was most frequently found in 27.5% of patients followed by endometrial carcinoma and vulvar carcinoma in 25% respectively. The final histopathologic results after surgery with IORT showed no residual tumour in 24 patients (60%), microscopic residual disease in 5 patients (12.5%), resection status could not be evaluated in three patients (7.5%) and the resection status was unknown in eight patients (20%). Subsequently, 27.5% of patients also received adjuvant radiotherapy of the local recurrence bed. However, after IORT, 65% of the women suffered a recurrence. Of these, the recurrences were localized: in-field 32.5%, out-of-field 22.5% and margin-of-field 12.5%. The 3- and 5-year OS was 69% and 55% respectively. The 3- and 5-year LRC was 56% respectively. The 3- and 5-year DMFS was 66% and 49%. Whereas the comparison between groups by IORT dose level (≤ 13 vs. >13 Gy) showed a non-significant trend in favor of the higher dose only for OS (p = 0.094), but not in LRC and DMFS (p > 0.05). OS and DMFS, but not LRC, differed significantly between the HDR-IORT and IOERT groups (p = 0.06 and p = 0.03,) in favor of the HDR-IORT technique. For HDR-IORT technique a trend towards superior OS and LRC was observed in the univariate analysis: HR 3.76, CI 95%: 0.95-14.881, p = 0.059 and HR 2.165 CI 95%: 0.916-5.114, p = 0.078 CONCLUSIONS: The survival rate for pelvic recurrence in gynecological malignancies remains poor and comparable with historical data from the last two decades. Particularly HDR-IORT, appears to provide a long-term oncological benefit in carefully selected patients.</p>\",\"PeriodicalId\":49639,\"journal\":{\"name\":\"Radiation Oncology\",\"volume\":\"19 1\",\"pages\":\"147\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515090/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13014-024-02537-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-024-02537-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
The value of a multimodal approach combining radical surgery and intraoperative radiotherapy in the recurrence treatment of gynecological malignancies - analysis of a large patient cohort in a tertiary care center.
Background: Recurrent and locally advanced gynecological malignancies have a poor prognosis. In particularly, pelvic local recurrence after previous radiotherapy and/or positive resection margins during surgical treatment for recurrent disease result in low survival rates. Consequently, locoregional control is of utmost importance in this cohort of patients. The aim of this study was to analyze treatment outcomes and determine prognostic factors for patients treated with surgery and intraoperative radiotherapy (IORT) for recurrent and locally advanced gynecological malignancies.
Methods: 40 patients who underwent surgical treatment and IORT between 2010 and 2022 were eligible for inclusion. The median follow-up time was 22 months. The outcomes measured were locoregional control (LRC), overall survival (OS), and survival without distant metastases (DMFS). The Cox proportional hazards model was used for univariate and multivariate analysis to assess the impact of patient variables and treatment factors on the endpoints mentioned. The following variables were analyzed: age at surgical treatment and IORT and initial diagnosis (< 65 vs. ≥65 years, each), disease-free interval (DFI) between initial diagnosis and first recurrence, DFI to surgical treatment and IORT, grading, histology, IORT dose (≤ 13 vs. >13 Gy) and technique (high dose radiotherapy (HDR) vs. IORT using electrons, (IOERT)). Survival curves were generated using the Kaplan-Meier method.
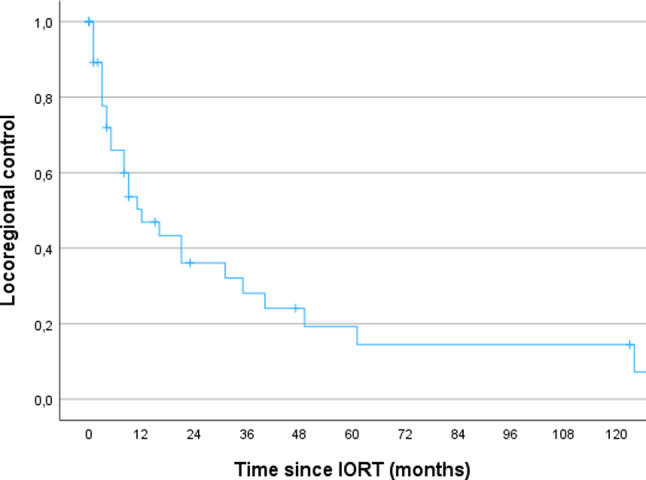
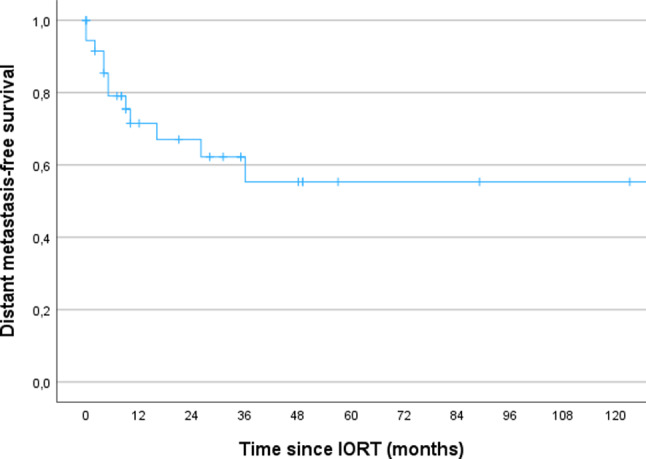
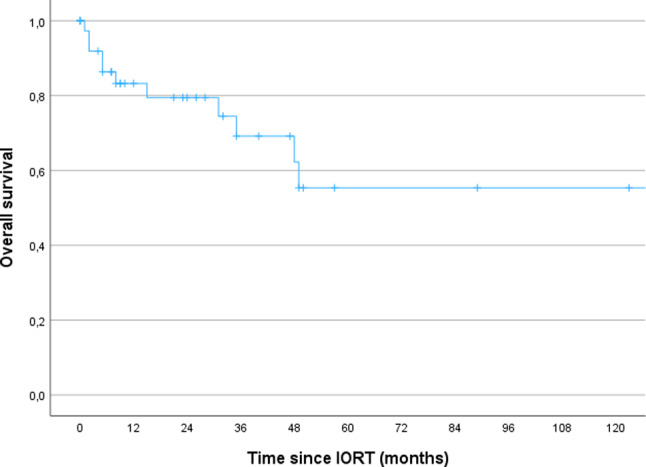
Results: The mean IORT dose was 13.8 Gy (range 10-18 Gy). Cervical carcinoma was most frequently found in 27.5% of patients followed by endometrial carcinoma and vulvar carcinoma in 25% respectively. The final histopathologic results after surgery with IORT showed no residual tumour in 24 patients (60%), microscopic residual disease in 5 patients (12.5%), resection status could not be evaluated in three patients (7.5%) and the resection status was unknown in eight patients (20%). Subsequently, 27.5% of patients also received adjuvant radiotherapy of the local recurrence bed. However, after IORT, 65% of the women suffered a recurrence. Of these, the recurrences were localized: in-field 32.5%, out-of-field 22.5% and margin-of-field 12.5%. The 3- and 5-year OS was 69% and 55% respectively. The 3- and 5-year LRC was 56% respectively. The 3- and 5-year DMFS was 66% and 49%. Whereas the comparison between groups by IORT dose level (≤ 13 vs. >13 Gy) showed a non-significant trend in favor of the higher dose only for OS (p = 0.094), but not in LRC and DMFS (p > 0.05). OS and DMFS, but not LRC, differed significantly between the HDR-IORT and IOERT groups (p = 0.06 and p = 0.03,) in favor of the HDR-IORT technique. For HDR-IORT technique a trend towards superior OS and LRC was observed in the univariate analysis: HR 3.76, CI 95%: 0.95-14.881, p = 0.059 and HR 2.165 CI 95%: 0.916-5.114, p = 0.078 CONCLUSIONS: The survival rate for pelvic recurrence in gynecological malignancies remains poor and comparable with historical data from the last two decades. Particularly HDR-IORT, appears to provide a long-term oncological benefit in carefully selected patients.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
