Timbre Backen, Kristin Salottolo, David Acuna, Carlos H Palacio, Gina Berg, Andrea Tsoris, Robert Madayag, Kaysie Banton, David Bar-Or
{"title":"多中心研究:利用连接点回归分析六年来创伤性颅内出血的时间趋势","authors":"Timbre Backen, Kristin Salottolo, David Acuna, Carlos H Palacio, Gina Berg, Andrea Tsoris, Robert Madayag, Kaysie Banton, David Bar-Or","doi":"10.1089/neur.2024.0097","DOIUrl":null,"url":null,"abstract":"<p><p>The aging US population has altered the epidemiology of traumatic injury, but there are few studies examining changing patterns of traumatic intracranial hemorrhage (tICH). We examined temporal changes in incidence, demographics, severity, management, and outcomes of tICH among trauma admissions at six US Level I trauma centers over 6 years (July 1, 2016-June 30, 2022). Patients with tICH (subdural, epidural, subarachnoid, and intracerebral hemorrhage) were identified by 10th revision of the International Statistical Classification of Diseases diagnosis codes. Temporal trends were examined over 12 six-month intervals using joinpoint regression and reported as biannual percent change (BPC); models without joinpoints are described as linear trends over time. There were 67,514 trauma admissions over 6 years and 11,935 (17.7%) patients had a tICH. The proportion of tICH injuries significantly increased 2.6% biannually from July 2016 to July 2019 (BPC = 2.6, <i>p</i> = 0.04), then leveled off through June 2022 (BPC = -0.9, <i>p</i> = 0.19). Similarly, the proportion of geriatric patients (≥65 years old) increased 2.4% biannually from July 2016 to July 2019 (BPC = 2.4, <i>p</i> = 0.001) as did injuries due to falls (BPC = 2.2, <i>p</i> = 0.01). Three of the four most prevalent comorbidities significantly increased: hypertension linearly increased 2.1% biannually, functional dependence increased 25.5% biannually through June 2019, and chronic anticoagulant use increased 19.0% biannually through June 2019 and then 3.1% thereafter. There were no trends in the rates of neurosurgical intervention (BPC = -0.89, <i>p</i> = 0.40), ED Glasgow coma score 3-8 (BPC = -0.4, <i>p</i> = 0.77), or presence of severe extracranial injuries (BPC = -0.7, <i>p</i> = 0.45). In-hospital mortality linearly declined 2.6% biannually (BPC = 2.6, <i>p</i> = 0.05); however, there was a 10.3% biannual linear increase in discharge to hospice care (BPC = 10.3, <i>p</i> < 0.001). These results demonstrate the incidence of tICH admissions is temporally increasing, and the population is growing older with more comorbidities and injuries from falls. Yet, traumatic brain injury severity and neurosurgical management are unchanged. The shift from in-patient death to hospice care suggests an increased need for palliative care services.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"5 1","pages":"999-1008"},"PeriodicalIF":1.7000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491587/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multicenter Study Examining Temporal Trends in Traumatic Intracranial Hemorrhage Over Six Years Using Joinpoint Regression.\",\"authors\":\"Timbre Backen, Kristin Salottolo, David Acuna, Carlos H Palacio, Gina Berg, Andrea Tsoris, Robert Madayag, Kaysie Banton, David Bar-Or\",\"doi\":\"10.1089/neur.2024.0097\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The aging US population has altered the epidemiology of traumatic injury, but there are few studies examining changing patterns of traumatic intracranial hemorrhage (tICH). We examined temporal changes in incidence, demographics, severity, management, and outcomes of tICH among trauma admissions at six US Level I trauma centers over 6 years (July 1, 2016-June 30, 2022). Patients with tICH (subdural, epidural, subarachnoid, and intracerebral hemorrhage) were identified by 10th revision of the International Statistical Classification of Diseases diagnosis codes. Temporal trends were examined over 12 six-month intervals using joinpoint regression and reported as biannual percent change (BPC); models without joinpoints are described as linear trends over time. There were 67,514 trauma admissions over 6 years and 11,935 (17.7%) patients had a tICH. The proportion of tICH injuries significantly increased 2.6% biannually from July 2016 to July 2019 (BPC = 2.6, <i>p</i> = 0.04), then leveled off through June 2022 (BPC = -0.9, <i>p</i> = 0.19). Similarly, the proportion of geriatric patients (≥65 years old) increased 2.4% biannually from July 2016 to July 2019 (BPC = 2.4, <i>p</i> = 0.001) as did injuries due to falls (BPC = 2.2, <i>p</i> = 0.01). Three of the four most prevalent comorbidities significantly increased: hypertension linearly increased 2.1% biannually, functional dependence increased 25.5% biannually through June 2019, and chronic anticoagulant use increased 19.0% biannually through June 2019 and then 3.1% thereafter. There were no trends in the rates of neurosurgical intervention (BPC = -0.89, <i>p</i> = 0.40), ED Glasgow coma score 3-8 (BPC = -0.4, <i>p</i> = 0.77), or presence of severe extracranial injuries (BPC = -0.7, <i>p</i> = 0.45). In-hospital mortality linearly declined 2.6% biannually (BPC = 2.6, <i>p</i> = 0.05); however, there was a 10.3% biannual linear increase in discharge to hospice care (BPC = 10.3, <i>p</i> < 0.001). These results demonstrate the incidence of tICH admissions is temporally increasing, and the population is growing older with more comorbidities and injuries from falls. Yet, traumatic brain injury severity and neurosurgical management are unchanged. The shift from in-patient death to hospice care suggests an increased need for palliative care services.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"5 1\",\"pages\":\"999-1008\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-10-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491587/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0097\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Multicenter Study Examining Temporal Trends in Traumatic Intracranial Hemorrhage Over Six Years Using Joinpoint Regression.
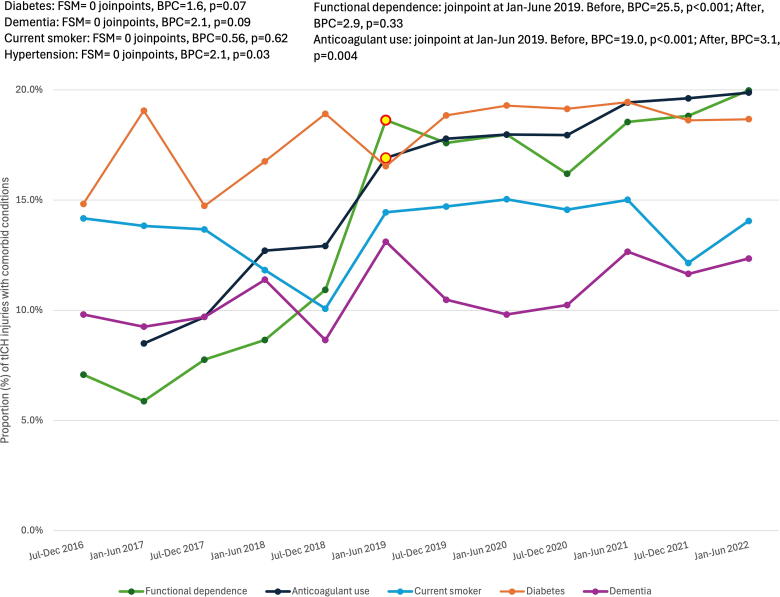
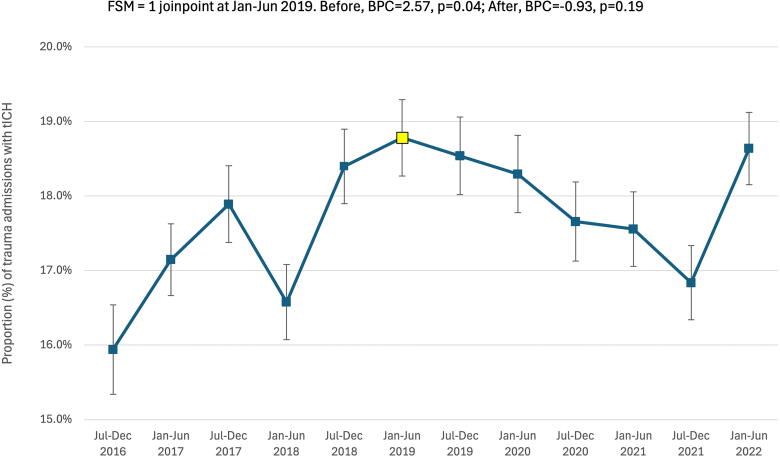
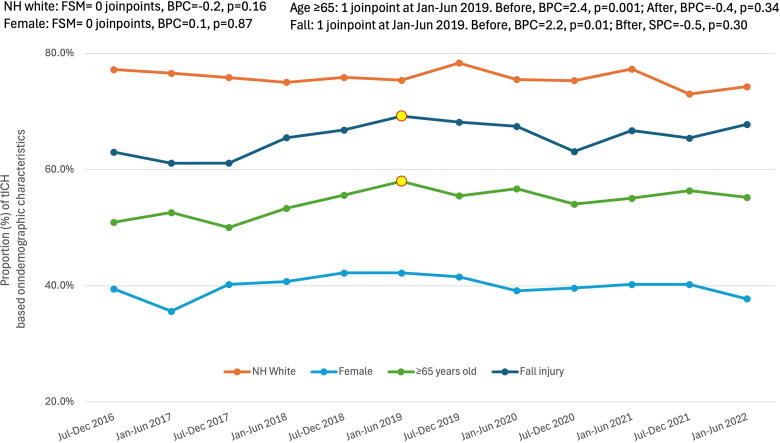
The aging US population has altered the epidemiology of traumatic injury, but there are few studies examining changing patterns of traumatic intracranial hemorrhage (tICH). We examined temporal changes in incidence, demographics, severity, management, and outcomes of tICH among trauma admissions at six US Level I trauma centers over 6 years (July 1, 2016-June 30, 2022). Patients with tICH (subdural, epidural, subarachnoid, and intracerebral hemorrhage) were identified by 10th revision of the International Statistical Classification of Diseases diagnosis codes. Temporal trends were examined over 12 six-month intervals using joinpoint regression and reported as biannual percent change (BPC); models without joinpoints are described as linear trends over time. There were 67,514 trauma admissions over 6 years and 11,935 (17.7%) patients had a tICH. The proportion of tICH injuries significantly increased 2.6% biannually from July 2016 to July 2019 (BPC = 2.6, p = 0.04), then leveled off through June 2022 (BPC = -0.9, p = 0.19). Similarly, the proportion of geriatric patients (≥65 years old) increased 2.4% biannually from July 2016 to July 2019 (BPC = 2.4, p = 0.001) as did injuries due to falls (BPC = 2.2, p = 0.01). Three of the four most prevalent comorbidities significantly increased: hypertension linearly increased 2.1% biannually, functional dependence increased 25.5% biannually through June 2019, and chronic anticoagulant use increased 19.0% biannually through June 2019 and then 3.1% thereafter. There were no trends in the rates of neurosurgical intervention (BPC = -0.89, p = 0.40), ED Glasgow coma score 3-8 (BPC = -0.4, p = 0.77), or presence of severe extracranial injuries (BPC = -0.7, p = 0.45). In-hospital mortality linearly declined 2.6% biannually (BPC = 2.6, p = 0.05); however, there was a 10.3% biannual linear increase in discharge to hospice care (BPC = 10.3, p < 0.001). These results demonstrate the incidence of tICH admissions is temporally increasing, and the population is growing older with more comorbidities and injuries from falls. Yet, traumatic brain injury severity and neurosurgical management are unchanged. The shift from in-patient death to hospice care suggests an increased need for palliative care services.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
