Eric N. Reed MD, Joan Papp MD, Yesol Oh MD, Kellie LeVine MD, Yasir Tarabichi MD, Estella Bastian BA, Kailee Pollock PharmD, Lance D. Wilson MD, Jonathan Siff MD, Joseph S. Piktel MD
{"title":"评估以急诊科为基础的减少后续阿片类药物过量的方法。","authors":"Eric N. Reed MD, Joan Papp MD, Yesol Oh MD, Kellie LeVine MD, Yasir Tarabichi MD, Estella Bastian BA, Kailee Pollock PharmD, Lance D. Wilson MD, Jonathan Siff MD, Joseph S. Piktel MD","doi":"10.1002/emp2.13304","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>The purpose of this study was to determine the association of a multi-pronged treatment program in emergency department (ED) patients with an acute presentation of opioid use disorder (OUD) on the rate of subsequent opioid overdose (OD). This approach included ED-initiated take-home naloxone, prescription buprenorphine, and an ED-based peer support and recovery program.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a retrospective observational analysis of adult patients presenting to the ED at a large urban hospital system from November 1, 2017 to March 17, 2023. Patients with an ED discharge diagnosis of OD or OUD were included. Outcomes determined were subsequent 90-day OD and 180-day OD death. Post hoc analyses were performed to identify intervention utilization throughout the study period including the COVID-19 pandemic as well as ED characteristics associated with subsequent OD and OD death. Statistical comparisons were made using logistic regression and chi-squared test.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 2634 patients presented to the ED with an opioid OD or diagnosis of OUD. Subsequent 90-day OD decreased significantly over time (11.5%–2.3%, odds ratio [OR] 0.85, confidence interval [CI] 0.82–0.89). No single intervention was independently associated with 90-day OD or 180-day OD death. Resource utilization was stable during the COVID-19 pandemic and increased afterward. A higher buprenorphine fill-rate among all patients and the Back race subgroup was associated with a decrease in 90-day OD.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Subsequent OD and OD death decreased over time after implementation of a multi-pronged treatment program to ED patients with OUD. No single intervention was associated with a decrease of subsequent OD or OD death.</p>\n </section>\n </div>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11496383/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of an emergency department-based approach to reduce subsequent opioid overdoses\",\"authors\":\"Eric N. Reed MD, Joan Papp MD, Yesol Oh MD, Kellie LeVine MD, Yasir Tarabichi MD, Estella Bastian BA, Kailee Pollock PharmD, Lance D. Wilson MD, Jonathan Siff MD, Joseph S. Piktel MD\",\"doi\":\"10.1002/emp2.13304\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>The purpose of this study was to determine the association of a multi-pronged treatment program in emergency department (ED) patients with an acute presentation of opioid use disorder (OUD) on the rate of subsequent opioid overdose (OD). This approach included ED-initiated take-home naloxone, prescription buprenorphine, and an ED-based peer support and recovery program.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a retrospective observational analysis of adult patients presenting to the ED at a large urban hospital system from November 1, 2017 to March 17, 2023. Patients with an ED discharge diagnosis of OD or OUD were included. Outcomes determined were subsequent 90-day OD and 180-day OD death. Post hoc analyses were performed to identify intervention utilization throughout the study period including the COVID-19 pandemic as well as ED characteristics associated with subsequent OD and OD death. Statistical comparisons were made using logistic regression and chi-squared test.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 2634 patients presented to the ED with an opioid OD or diagnosis of OUD. Subsequent 90-day OD decreased significantly over time (11.5%–2.3%, odds ratio [OR] 0.85, confidence interval [CI] 0.82–0.89). No single intervention was independently associated with 90-day OD or 180-day OD death. Resource utilization was stable during the COVID-19 pandemic and increased afterward. A higher buprenorphine fill-rate among all patients and the Back race subgroup was associated with a decrease in 90-day OD.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Subsequent OD and OD death decreased over time after implementation of a multi-pronged treatment program to ED patients with OUD. No single intervention was associated with a decrease of subsequent OD or OD death.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73967,\"journal\":{\"name\":\"Journal of the American College of Emergency Physicians open\",\"volume\":\"5 5\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-10-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11496383/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Emergency Physicians open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13304\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13304","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
研究目的本研究旨在确定急诊科(ED)急性阿片类药物使用障碍(OUD)患者多管齐下的治疗方案与后续阿片类药物过量(OD)发生率的关系。这种方法包括由急诊科发起的带回家纳洛酮、处方丁丙诺啡以及基于急诊科的同伴支持和康复计划:这是一项回顾性观察分析,研究对象是 2017 年 11 月 1 日至 2023 年 3 月 17 日在一家大型城市医院系统就诊的 ED 成人患者。纳入的患者出院诊断为 OD 或 OUD。确定的结果是随后90天的OD和180天的OD死亡。进行了事后分析,以确定整个研究期间的干预利用情况,包括 COVID-19 大流行以及与后续 OD 和 OD 死亡相关的 ED 特征。统计比较采用逻辑回归和卡方检验:共有 2634 名患者因阿片类药物过量或被诊断为 OUD 而就诊于急诊室。随着时间的推移,其后90天的OD明显减少(11.5%-2.3%,几率比[OR]0.85,置信区间[CI]0.82-0.89)。没有任何一项干预措施与 90 天 OD 或 180 天 OD 死亡独立相关。在 COVID-19 大流行期间,资源利用率保持稳定,而在大流行之后则有所上升。在所有患者和背部种族亚组中,较高的丁丙诺啡填充率与90天OD下降有关:结论:在对患有 OUD 的 ED 患者实施多管齐下的治疗计划后,其后的 OD 和 OD 死亡人数随时间推移而减少。没有任何一项干预措施与后续OD或OD死亡的减少有关。
Evaluation of an emergency department-based approach to reduce subsequent opioid overdoses
Objective
The purpose of this study was to determine the association of a multi-pronged treatment program in emergency department (ED) patients with an acute presentation of opioid use disorder (OUD) on the rate of subsequent opioid overdose (OD). This approach included ED-initiated take-home naloxone, prescription buprenorphine, and an ED-based peer support and recovery program.
Methods
This was a retrospective observational analysis of adult patients presenting to the ED at a large urban hospital system from November 1, 2017 to March 17, 2023. Patients with an ED discharge diagnosis of OD or OUD were included. Outcomes determined were subsequent 90-day OD and 180-day OD death. Post hoc analyses were performed to identify intervention utilization throughout the study period including the COVID-19 pandemic as well as ED characteristics associated with subsequent OD and OD death. Statistical comparisons were made using logistic regression and chi-squared test.
Results
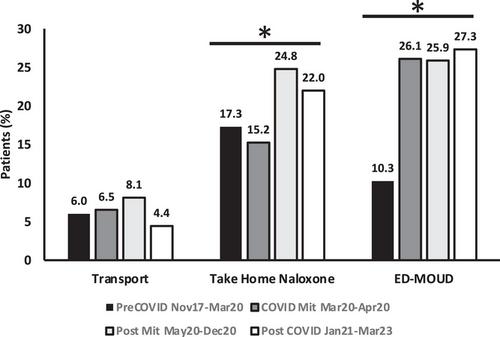
A total of 2634 patients presented to the ED with an opioid OD or diagnosis of OUD. Subsequent 90-day OD decreased significantly over time (11.5%–2.3%, odds ratio [OR] 0.85, confidence interval [CI] 0.82–0.89). No single intervention was independently associated with 90-day OD or 180-day OD death. Resource utilization was stable during the COVID-19 pandemic and increased afterward. A higher buprenorphine fill-rate among all patients and the Back race subgroup was associated with a decrease in 90-day OD.
Conclusions
Subsequent OD and OD death decreased over time after implementation of a multi-pronged treatment program to ED patients with OUD. No single intervention was associated with a decrease of subsequent OD or OD death.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
