Emily Newton-Hoe, Alisa B Goldberg, Jennifer Fortin, Elizabeth Janiak, Sara Neill
{"title":"马萨诸塞州妇产科医生使用米非司酮治疗早期流产和人工流产的空间差异。","authors":"Emily Newton-Hoe, Alisa B Goldberg, Jennifer Fortin, Elizabeth Janiak, Sara Neill","doi":"10.1089/whr.2024.0085","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>About 25% of pregnancies end in early miscarriage or abortion annually in the United States. While mifepristone is part of the most effective medication regimen for miscarriage and abortion, regulatory burdens and legal restrictions limit its provision in obstetric-gynecological practice. The extent of geographic disparities in mifepristone use is unknown.</p><p><strong>Objectives: </strong>We sought to ascertain whether regional \"deserts\" for mifepristone-based miscarriage and abortion care exist in Massachusetts using geographic regions specified by the Commonwealth's Executive Office of Health and Human Services.</p><p><strong>Methods: </strong>We fielded a cross-sectional survey of obstetrician-gynecologists practicing in Massachusetts. We weighted survey data to account for differential nonresponse by provider sex, region, and years in independent practice.</p><p><strong>Results: </strong>Among obstetrician-gynecologists in independent practice with region data (<i>n</i> = 148), 51.0% reported using mifepristone for miscarriage and 43.5% for abortion. Significant differences in reported use were observed across regions (<i>p</i> < 0.001 for both indications). Barriers to using mifepristone for miscarriage management also varied across regions. Respondents outside of Boston and Western Massachusetts were more likely to report gaps in knowledge about regulations and prescribing and had less prior experience using mifepristone. In a multivariable model adjusting for provider sex and practice type, obstetrician-gynecologists outside of Boston had significantly lower odds of using mifepristone for miscarriage (adjusted odds ratio [aOR] = 0.14, 95% confidence interval [95% CI] = 0.08-0.25) and abortion (aOR = 0.46, 95% CI = 0.26-0.82), compared to Boston-based obstetrician-gynecologists.</p><p><strong>Conclusion: </strong>Mifepristone provision varies significantly by Massachusetts region. This may lead to spatial disparities in reproductive health outcomes.</p>","PeriodicalId":75329,"journal":{"name":"Women's health reports (New Rochelle, N.Y.)","volume":"5 1","pages":"765-774"},"PeriodicalIF":1.8000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491581/pdf/","citationCount":"0","resultStr":"{\"title\":\"Spatial Disparities in Mifepristone Use for Early Miscarriage and Induced Abortion Among Obstetrician-Gynecologists Practicing in Massachusetts.\",\"authors\":\"Emily Newton-Hoe, Alisa B Goldberg, Jennifer Fortin, Elizabeth Janiak, Sara Neill\",\"doi\":\"10.1089/whr.2024.0085\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>About 25% of pregnancies end in early miscarriage or abortion annually in the United States. While mifepristone is part of the most effective medication regimen for miscarriage and abortion, regulatory burdens and legal restrictions limit its provision in obstetric-gynecological practice. The extent of geographic disparities in mifepristone use is unknown.</p><p><strong>Objectives: </strong>We sought to ascertain whether regional \\\"deserts\\\" for mifepristone-based miscarriage and abortion care exist in Massachusetts using geographic regions specified by the Commonwealth's Executive Office of Health and Human Services.</p><p><strong>Methods: </strong>We fielded a cross-sectional survey of obstetrician-gynecologists practicing in Massachusetts. We weighted survey data to account for differential nonresponse by provider sex, region, and years in independent practice.</p><p><strong>Results: </strong>Among obstetrician-gynecologists in independent practice with region data (<i>n</i> = 148), 51.0% reported using mifepristone for miscarriage and 43.5% for abortion. Significant differences in reported use were observed across regions (<i>p</i> < 0.001 for both indications). Barriers to using mifepristone for miscarriage management also varied across regions. Respondents outside of Boston and Western Massachusetts were more likely to report gaps in knowledge about regulations and prescribing and had less prior experience using mifepristone. In a multivariable model adjusting for provider sex and practice type, obstetrician-gynecologists outside of Boston had significantly lower odds of using mifepristone for miscarriage (adjusted odds ratio [aOR] = 0.14, 95% confidence interval [95% CI] = 0.08-0.25) and abortion (aOR = 0.46, 95% CI = 0.26-0.82), compared to Boston-based obstetrician-gynecologists.</p><p><strong>Conclusion: </strong>Mifepristone provision varies significantly by Massachusetts region. This may lead to spatial disparities in reproductive health outcomes.</p>\",\"PeriodicalId\":75329,\"journal\":{\"name\":\"Women's health reports (New Rochelle, N.Y.)\",\"volume\":\"5 1\",\"pages\":\"765-774\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491581/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Women's health reports (New Rochelle, N.Y.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/whr.2024.0085\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health reports (New Rochelle, N.Y.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/whr.2024.0085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Spatial Disparities in Mifepristone Use for Early Miscarriage and Induced Abortion Among Obstetrician-Gynecologists Practicing in Massachusetts.
Background: About 25% of pregnancies end in early miscarriage or abortion annually in the United States. While mifepristone is part of the most effective medication regimen for miscarriage and abortion, regulatory burdens and legal restrictions limit its provision in obstetric-gynecological practice. The extent of geographic disparities in mifepristone use is unknown.
Objectives: We sought to ascertain whether regional "deserts" for mifepristone-based miscarriage and abortion care exist in Massachusetts using geographic regions specified by the Commonwealth's Executive Office of Health and Human Services.
Methods: We fielded a cross-sectional survey of obstetrician-gynecologists practicing in Massachusetts. We weighted survey data to account for differential nonresponse by provider sex, region, and years in independent practice.
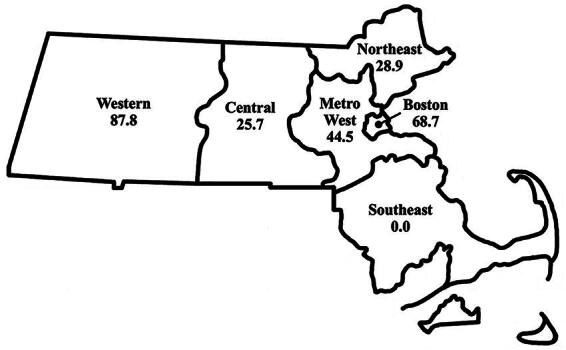
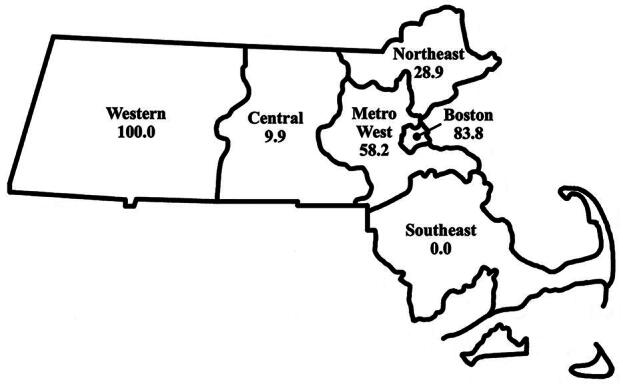
Results: Among obstetrician-gynecologists in independent practice with region data (n = 148), 51.0% reported using mifepristone for miscarriage and 43.5% for abortion. Significant differences in reported use were observed across regions (p < 0.001 for both indications). Barriers to using mifepristone for miscarriage management also varied across regions. Respondents outside of Boston and Western Massachusetts were more likely to report gaps in knowledge about regulations and prescribing and had less prior experience using mifepristone. In a multivariable model adjusting for provider sex and practice type, obstetrician-gynecologists outside of Boston had significantly lower odds of using mifepristone for miscarriage (adjusted odds ratio [aOR] = 0.14, 95% confidence interval [95% CI] = 0.08-0.25) and abortion (aOR = 0.46, 95% CI = 0.26-0.82), compared to Boston-based obstetrician-gynecologists.
Conclusion: Mifepristone provision varies significantly by Massachusetts region. This may lead to spatial disparities in reproductive health outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
