Lauriane Guichard, Milo C Engoren, Yi-Ju Li, Matthew J Sigakis, Xinming An, Chad M Brummett, Matthew C Mauck, Karthik Raghunathan, Daniel J Clauw, Vijay Krishnamoorthy
{"title":"术后重症监护期间阿片类药物使用增加的风险因素。","authors":"Lauriane Guichard, Milo C Engoren, Yi-Ju Li, Matthew J Sigakis, Xinming An, Chad M Brummett, Matthew C Mauck, Karthik Raghunathan, Daniel J Clauw, Vijay Krishnamoorthy","doi":"10.1097/CCE.0000000000001172","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>In the ICU, opioids treat pain and improve ventilator tolerance as part of an analgosedation approach. Identifying predictors of opioid consumption during the ICU course might highlight actionable items to reduce opioid consumption.</p><p><strong>Objectives: </strong>To identify risk factors for opioid use during a postoperative ICU course.</p><p><strong>Design, setting, and participants: </strong>Patients enrolled in the Michigan Genomics Initiative single-center prospective observational cohort study completed baseline preoperative sociodemographic and mental/physical health questionnaires and provided blood samples for genetic analysis. Included patients were 18 years old and older, admitted to ICU postoperatively, and received opioids postoperatively.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was ICU mean daily oral morphine equivalent (OME) use. The association between OME and phenotypic risk factors and genetic variants previously associated with pain were analyzed through univariable and multivariable linear regression models.</p><p><strong>Results: </strong>The cohort consisted of 1865 mixed-surgical patients with mean age of 56 years (sd, 15 yr). Preoperative opioid users were more likely to continue to receive opioids throughout their ICU stay than opioid-naive patients. OME (log10 scale) was most strongly associated with ICU mechanical ventilation (β = 0.27; 95% CI, 0.15-0.38; p < 0.0001; effect size 1.85 for receiving > 24 hours of mechanical ventilation), preoperative opioid use (β = 0.22; 95% CI, 0.16-0.29; p < 0.0001; effect size 1.67 for receiving preoperative opioids), major surgery (β = 0.21; 95% CI, 0.12-0.30; p < 0.0001; effect size 1.62 compared with minor surgery), and current/former illicit drug use (β = 0.12; 95% CI, 0.01-0.23; p = 0.04; effect size 1.30 for drug use). Younger age, centralized pain, and longer anesthetic duration were also significantly associated with OME but with smaller effect sizes. Selected genetic variants (FKBP5, COMT, and OPRM1) were not associated with OME use.</p><p><strong>Conclusions and relevance: </strong>Mechanical ventilation and preoperative opioids were the strongest risk factors for postoperative ICU opioid consumption, whereas psychologic factors and genetic variants were not associated.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 11","pages":"e1172"},"PeriodicalIF":2.7000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11519407/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors for Increased Opioid Use During Postoperative Intensive Care.\",\"authors\":\"Lauriane Guichard, Milo C Engoren, Yi-Ju Li, Matthew J Sigakis, Xinming An, Chad M Brummett, Matthew C Mauck, Karthik Raghunathan, Daniel J Clauw, Vijay Krishnamoorthy\",\"doi\":\"10.1097/CCE.0000000000001172\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>In the ICU, opioids treat pain and improve ventilator tolerance as part of an analgosedation approach. Identifying predictors of opioid consumption during the ICU course might highlight actionable items to reduce opioid consumption.</p><p><strong>Objectives: </strong>To identify risk factors for opioid use during a postoperative ICU course.</p><p><strong>Design, setting, and participants: </strong>Patients enrolled in the Michigan Genomics Initiative single-center prospective observational cohort study completed baseline preoperative sociodemographic and mental/physical health questionnaires and provided blood samples for genetic analysis. Included patients were 18 years old and older, admitted to ICU postoperatively, and received opioids postoperatively.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was ICU mean daily oral morphine equivalent (OME) use. The association between OME and phenotypic risk factors and genetic variants previously associated with pain were analyzed through univariable and multivariable linear regression models.</p><p><strong>Results: </strong>The cohort consisted of 1865 mixed-surgical patients with mean age of 56 years (sd, 15 yr). Preoperative opioid users were more likely to continue to receive opioids throughout their ICU stay than opioid-naive patients. OME (log10 scale) was most strongly associated with ICU mechanical ventilation (β = 0.27; 95% CI, 0.15-0.38; p < 0.0001; effect size 1.85 for receiving > 24 hours of mechanical ventilation), preoperative opioid use (β = 0.22; 95% CI, 0.16-0.29; p < 0.0001; effect size 1.67 for receiving preoperative opioids), major surgery (β = 0.21; 95% CI, 0.12-0.30; p < 0.0001; effect size 1.62 compared with minor surgery), and current/former illicit drug use (β = 0.12; 95% CI, 0.01-0.23; p = 0.04; effect size 1.30 for drug use). Younger age, centralized pain, and longer anesthetic duration were also significantly associated with OME but with smaller effect sizes. Selected genetic variants (FKBP5, COMT, and OPRM1) were not associated with OME use.</p><p><strong>Conclusions and relevance: </strong>Mechanical ventilation and preoperative opioids were the strongest risk factors for postoperative ICU opioid consumption, whereas psychologic factors and genetic variants were not associated.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"6 11\",\"pages\":\"e1172\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11519407/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001172\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001172","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Risk Factors for Increased Opioid Use During Postoperative Intensive Care.
Importance: In the ICU, opioids treat pain and improve ventilator tolerance as part of an analgosedation approach. Identifying predictors of opioid consumption during the ICU course might highlight actionable items to reduce opioid consumption.
Objectives: To identify risk factors for opioid use during a postoperative ICU course.
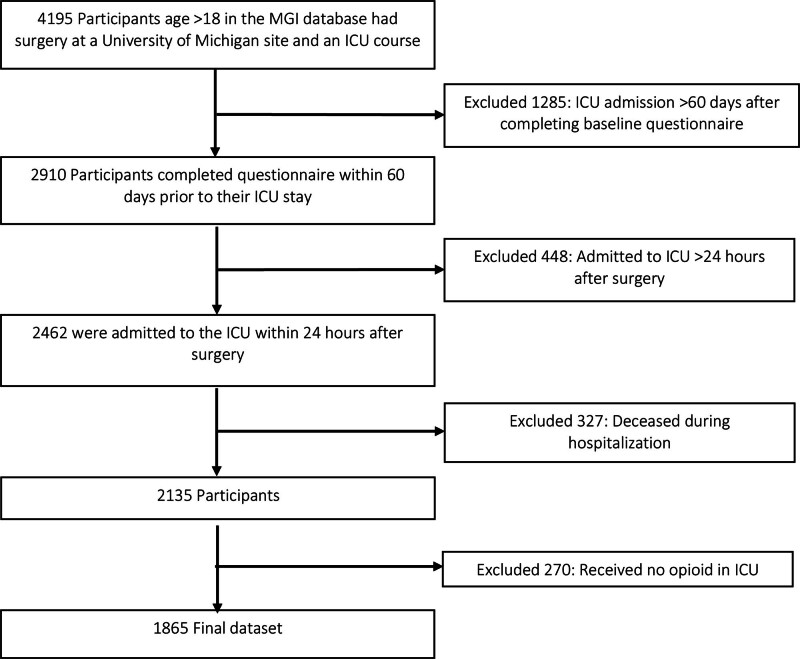
Design, setting, and participants: Patients enrolled in the Michigan Genomics Initiative single-center prospective observational cohort study completed baseline preoperative sociodemographic and mental/physical health questionnaires and provided blood samples for genetic analysis. Included patients were 18 years old and older, admitted to ICU postoperatively, and received opioids postoperatively.
Main outcomes and measures: The primary outcome was ICU mean daily oral morphine equivalent (OME) use. The association between OME and phenotypic risk factors and genetic variants previously associated with pain were analyzed through univariable and multivariable linear regression models.
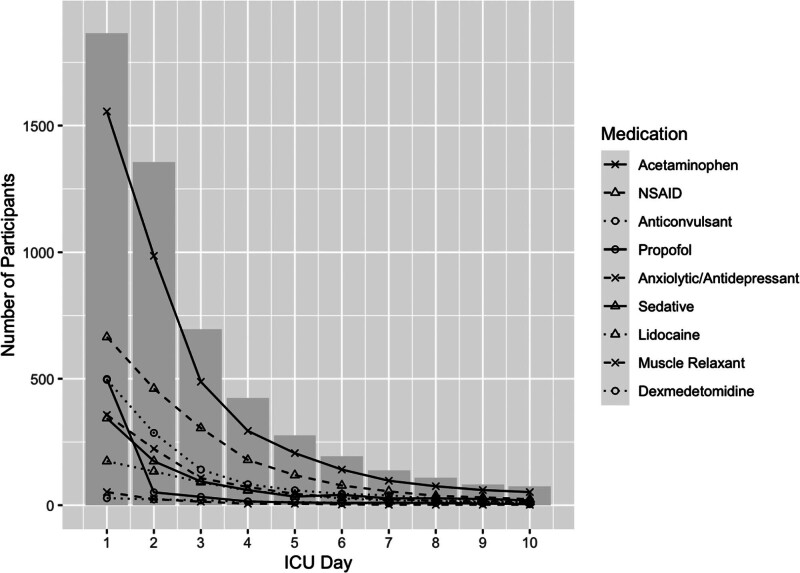
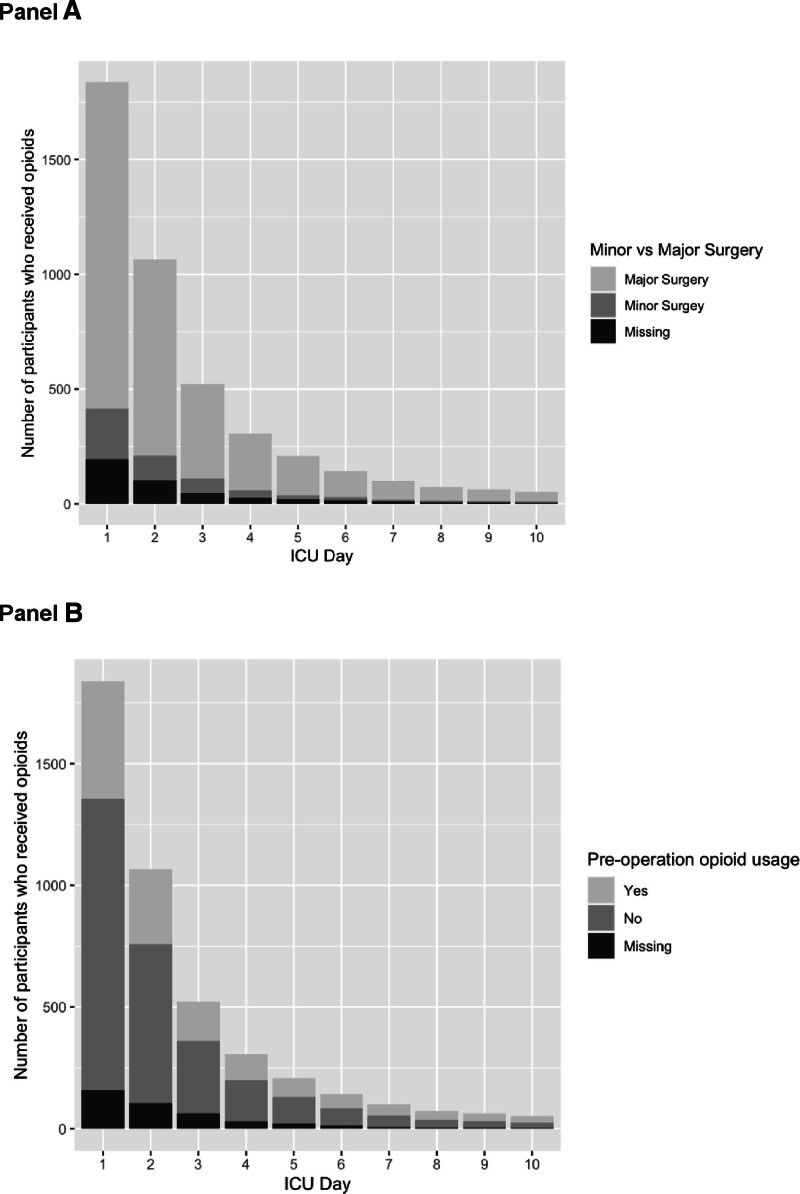
Results: The cohort consisted of 1865 mixed-surgical patients with mean age of 56 years (sd, 15 yr). Preoperative opioid users were more likely to continue to receive opioids throughout their ICU stay than opioid-naive patients. OME (log10 scale) was most strongly associated with ICU mechanical ventilation (β = 0.27; 95% CI, 0.15-0.38; p < 0.0001; effect size 1.85 for receiving > 24 hours of mechanical ventilation), preoperative opioid use (β = 0.22; 95% CI, 0.16-0.29; p < 0.0001; effect size 1.67 for receiving preoperative opioids), major surgery (β = 0.21; 95% CI, 0.12-0.30; p < 0.0001; effect size 1.62 compared with minor surgery), and current/former illicit drug use (β = 0.12; 95% CI, 0.01-0.23; p = 0.04; effect size 1.30 for drug use). Younger age, centralized pain, and longer anesthetic duration were also significantly associated with OME but with smaller effect sizes. Selected genetic variants (FKBP5, COMT, and OPRM1) were not associated with OME use.
Conclusions and relevance: Mechanical ventilation and preoperative opioids were the strongest risk factors for postoperative ICU opioid consumption, whereas psychologic factors and genetic variants were not associated.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
