Furong Bai, Mingliang Yi, Min Cai, Cong Zhao, Xujie Jiang, Hong Yin
{"title":"经食道肺部超声引导下的可视肺募集操作对胸腔镜肺叶切除术后肺不张的影响:一项随机、单盲、前瞻性研究。","authors":"Furong Bai, Mingliang Yi, Min Cai, Cong Zhao, Xujie Jiang, Hong Yin","doi":"10.1186/s12871-024-02777-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although the incidence of postoperative atelectasis could be reduced using lung recruitment manoeuvres, it remains high. We hypothesised that intraoperative visual lung recruitment guided by trans-oesophageal lung ultrasound would be more effective than the conventional method for managing postoperative atelectasis.</p><p><strong>Methods: </strong>In this randomised, controlled, prospective study, 84 patients undergoing thoracoscopic lobectomy were recruited from Affiliated Chengdu Fifth People<sup>'</sup>s Hospital (teaching hospital) in China. Patients were grouped into trans-oesophageal lung ultrasound-guided (Group G, n = 42) and control (Group C, n = 42) groups.</p><p><strong>Methods: </strong>Lung recruitment was performed after anaesthesia induction, before chest closure and before the endotracheal tube extubation. In Group C, recruitment pressure was controlled at 30 cm H<sub>2</sub>O for 10 s (performed thrice); in Group G, the pressure was controlled at 30 cm H<sub>2</sub>O (performed thrice), and the tidal volume did not exceed 20 ml kg<sup>-1</sup> until no atelectasis was detected by trans-oesophageal ultrasound. The primary outcome was lung ultrasound scores measured at the post anaesthesia care unit 30 min after extubation. The secondary outcomes included the oxygenation index (30 min after extubation) and the incidence of atelectasis (30 min after extubation and 3 days after surgery).</p><p><strong>Results: </strong>The final analysis included 79 patients. The lung ultrasound score was significantly higher in the control group than in the ultrasound-guided group 30 min after extubation (Group C vs. Group G, 8.6 ± 2.6 vs. 6.5 ± 2.0, P < 0.001). No significant difference in the oxygenation indexes 30 min after extubation was observed between the groups (P = 0.074); however, the incidence of atelectasis 30 min after extubation significantly differed between the two groups (Group C vs. Group G, 57% vs. 33%, P = 0.031). The incidence of atelectasis 3 days after surgery did not significantly differ between the two groups (Group C vs. Group G, 45% vs. 28%, P = 0.122).</p><p><strong>Conclusions: </strong>Lung recruitment guided by trans-oesophageal lung ultrasound can reduce lung ultrasound scores and the incidence of atelectasis at the post anaesthesia care unit 30 min after extubation. However, it does not significantly reduce the incidence of atelectasis 3 days after surgery. TRIAL REGISTRATION: Registration number: ChiCTR2200062509. Registered on 10 /8/ 2022.</p>","PeriodicalId":9190,"journal":{"name":"BMC Anesthesiology","volume":"24 1","pages":"388"},"PeriodicalIF":2.6000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11514961/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of visual lung recruitment manoeuvres guided by trans-oesophageal lung ultrasound on atelectasis after thoracoscopic lobectomy: a randomised, single-blind, prospective study.\",\"authors\":\"Furong Bai, Mingliang Yi, Min Cai, Cong Zhao, Xujie Jiang, Hong Yin\",\"doi\":\"10.1186/s12871-024-02777-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although the incidence of postoperative atelectasis could be reduced using lung recruitment manoeuvres, it remains high. We hypothesised that intraoperative visual lung recruitment guided by trans-oesophageal lung ultrasound would be more effective than the conventional method for managing postoperative atelectasis.</p><p><strong>Methods: </strong>In this randomised, controlled, prospective study, 84 patients undergoing thoracoscopic lobectomy were recruited from Affiliated Chengdu Fifth People<sup>'</sup>s Hospital (teaching hospital) in China. Patients were grouped into trans-oesophageal lung ultrasound-guided (Group G, n = 42) and control (Group C, n = 42) groups.</p><p><strong>Methods: </strong>Lung recruitment was performed after anaesthesia induction, before chest closure and before the endotracheal tube extubation. In Group C, recruitment pressure was controlled at 30 cm H<sub>2</sub>O for 10 s (performed thrice); in Group G, the pressure was controlled at 30 cm H<sub>2</sub>O (performed thrice), and the tidal volume did not exceed 20 ml kg<sup>-1</sup> until no atelectasis was detected by trans-oesophageal ultrasound. The primary outcome was lung ultrasound scores measured at the post anaesthesia care unit 30 min after extubation. The secondary outcomes included the oxygenation index (30 min after extubation) and the incidence of atelectasis (30 min after extubation and 3 days after surgery).</p><p><strong>Results: </strong>The final analysis included 79 patients. The lung ultrasound score was significantly higher in the control group than in the ultrasound-guided group 30 min after extubation (Group C vs. Group G, 8.6 ± 2.6 vs. 6.5 ± 2.0, P < 0.001). No significant difference in the oxygenation indexes 30 min after extubation was observed between the groups (P = 0.074); however, the incidence of atelectasis 30 min after extubation significantly differed between the two groups (Group C vs. Group G, 57% vs. 33%, P = 0.031). The incidence of atelectasis 3 days after surgery did not significantly differ between the two groups (Group C vs. Group G, 45% vs. 28%, P = 0.122).</p><p><strong>Conclusions: </strong>Lung recruitment guided by trans-oesophageal lung ultrasound can reduce lung ultrasound scores and the incidence of atelectasis at the post anaesthesia care unit 30 min after extubation. However, it does not significantly reduce the incidence of atelectasis 3 days after surgery. TRIAL REGISTRATION: Registration number: ChiCTR2200062509. Registered on 10 /8/ 2022.</p>\",\"PeriodicalId\":9190,\"journal\":{\"name\":\"BMC Anesthesiology\",\"volume\":\"24 1\",\"pages\":\"388\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-10-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11514961/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Anesthesiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12871-024-02777-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12871-024-02777-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:虽然使用肺募集操作可以降低术后肺不张的发生率,但其发生率仍然很高。我们假设,在经食道肺部超声引导下进行术中可视化肺募集会比传统方法更有效地控制术后肺不张:在这项随机对照的前瞻性研究中,84名接受胸腔镜肺叶切除术的患者来自中国成都第五人民医院附属医院(教学医院)。患者被分为经食道肺超声引导组(G 组,42 人)和对照组(C 组,42 人):方法:在麻醉诱导后、关闭胸腔前和拔除气管插管前进行肺部吸引。在 C 组中,扩容压力控制在 30 cm H2O,持续 10 秒(共进行三次);在 G 组中,扩容压力控制在 30 cm H2O(共进行三次),潮气量不超过 20 ml kg-1,直至经食道超声检查未发现肺不张。主要结果是拔管后 30 分钟在麻醉后护理病房测量的肺部超声评分。次要结果包括氧合指数(拔管后 30 分钟)和肺不张发生率(拔管后 30 分钟和术后 3 天):最终分析包括 79 名患者。拔管 30 分钟后,对照组的肺部超声评分明显高于超声引导组(C 组 vs. G 组,8.6 ± 2.6 vs. 6.5 ± 2.0,P 结论:超声引导下的肺通气指数(拔管 30 分钟后和术后 3 天)和肺不张发生率(拔管 30 分钟后和术后 3 天)均高于对照组:经食道肺部超声引导下的肺募集可降低拔管后 30 分钟在麻醉后监护室的肺部超声评分和肺不张发生率。然而,它并不能显著降低术后 3 天的肺不张发生率。试验注册: 注册号:ChiCTR2200062509ChiCTR2200062509。注册日期:2022 年 8 月 10 日。
Effect of visual lung recruitment manoeuvres guided by trans-oesophageal lung ultrasound on atelectasis after thoracoscopic lobectomy: a randomised, single-blind, prospective study.
Background: Although the incidence of postoperative atelectasis could be reduced using lung recruitment manoeuvres, it remains high. We hypothesised that intraoperative visual lung recruitment guided by trans-oesophageal lung ultrasound would be more effective than the conventional method for managing postoperative atelectasis.
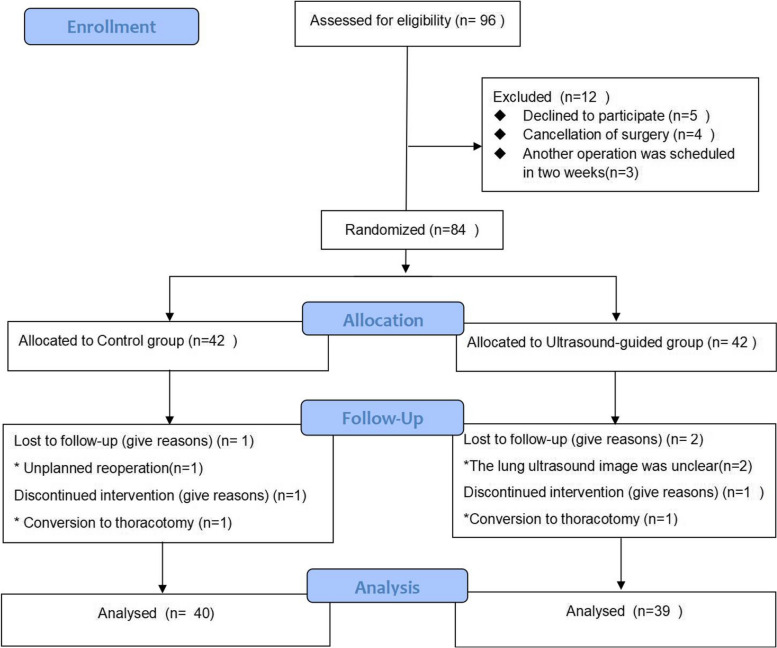
Methods: In this randomised, controlled, prospective study, 84 patients undergoing thoracoscopic lobectomy were recruited from Affiliated Chengdu Fifth People's Hospital (teaching hospital) in China. Patients were grouped into trans-oesophageal lung ultrasound-guided (Group G, n = 42) and control (Group C, n = 42) groups.
Methods: Lung recruitment was performed after anaesthesia induction, before chest closure and before the endotracheal tube extubation. In Group C, recruitment pressure was controlled at 30 cm H2O for 10 s (performed thrice); in Group G, the pressure was controlled at 30 cm H2O (performed thrice), and the tidal volume did not exceed 20 ml kg-1 until no atelectasis was detected by trans-oesophageal ultrasound. The primary outcome was lung ultrasound scores measured at the post anaesthesia care unit 30 min after extubation. The secondary outcomes included the oxygenation index (30 min after extubation) and the incidence of atelectasis (30 min after extubation and 3 days after surgery).
Results: The final analysis included 79 patients. The lung ultrasound score was significantly higher in the control group than in the ultrasound-guided group 30 min after extubation (Group C vs. Group G, 8.6 ± 2.6 vs. 6.5 ± 2.0, P < 0.001). No significant difference in the oxygenation indexes 30 min after extubation was observed between the groups (P = 0.074); however, the incidence of atelectasis 30 min after extubation significantly differed between the two groups (Group C vs. Group G, 57% vs. 33%, P = 0.031). The incidence of atelectasis 3 days after surgery did not significantly differ between the two groups (Group C vs. Group G, 45% vs. 28%, P = 0.122).
Conclusions: Lung recruitment guided by trans-oesophageal lung ultrasound can reduce lung ultrasound scores and the incidence of atelectasis at the post anaesthesia care unit 30 min after extubation. However, it does not significantly reduce the incidence of atelectasis 3 days after surgery. TRIAL REGISTRATION: Registration number: ChiCTR2200062509. Registered on 10 /8/ 2022.
期刊介绍:
BMC Anesthesiology is an open access, peer-reviewed journal that considers articles on all aspects of anesthesiology, critical care, perioperative care and pain management, including clinical and experimental research into anesthetic mechanisms, administration and efficacy, technology and monitoring, and associated economic issues.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
