Émilie Kate Landry, Annie Le-Nguyen, Elissa K Butler, Sarah Bouchard, Josée Dubois, Caroline P Lemoine
{"title":"胆总管囊肿和右侧先天性膈疝:何时干预?","authors":"Émilie Kate Landry, Annie Le-Nguyen, Elissa K Butler, Sarah Bouchard, Josée Dubois, Caroline P Lemoine","doi":"10.1055/s-0044-1791813","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with congenital diaphragmatic hernia (CDH) can present with other congenital anomalies, but an associated choledochal cyst (CC) has rarely been described. The simultaneous diagnosis of both anomalies complicates patient management. There is no consensus on the ideal timing for CC excision. Unrepaired CC is associated with risks of developing biliary sludge, choledocholithiasis, and cholangitis. After a CDH repair with mesh, secondary bacterial translocation caused by a delayed CC repair could lead to mesh superinfection. Conversely, early CC surgical management could cause mesh displacement and lead to CDH recurrence, requiring reintervention. We present the rare case of a CC occurring in a neonate with a prenatally diagnosed right CDH. One month after an uncomplicated CDH repair with mesh, while the patient was still hospitalized for pulmonary hypertension, she developed progressive cholestasis and acholic stools. Investigations revealed a nonpreviously suspected CC. Conservative treatment was attempted, but CC perforation with secondary biliary peritonitis occurred. Open CC excision with a Roux-en-Y hepaticojejunostomy was therefore performed on day of life (DOL) 41. Having suffered no short-term surgical complications, the patient was discharged on DOL 83 because of prolonged ventilatory support due to pulmonary hypertension. Now 12 months after surgery, she is doing well with normal liver function tests and imaging studies. In summary, CC should be considered in the differential diagnosis of progressive cholestasis in patients with CDH. Surgical repair of a symptomatic CC should not be delayed even in the presence of mesh given the risks of CC complications.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"12 1","pages":"e68-e72"},"PeriodicalIF":0.7000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11518628/pdf/","citationCount":"0","resultStr":"{\"title\":\"Choledochal Cyst and Right Congenital Diaphragmatic Hernia: When to Intervene?\",\"authors\":\"Émilie Kate Landry, Annie Le-Nguyen, Elissa K Butler, Sarah Bouchard, Josée Dubois, Caroline P Lemoine\",\"doi\":\"10.1055/s-0044-1791813\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patients with congenital diaphragmatic hernia (CDH) can present with other congenital anomalies, but an associated choledochal cyst (CC) has rarely been described. The simultaneous diagnosis of both anomalies complicates patient management. There is no consensus on the ideal timing for CC excision. Unrepaired CC is associated with risks of developing biliary sludge, choledocholithiasis, and cholangitis. After a CDH repair with mesh, secondary bacterial translocation caused by a delayed CC repair could lead to mesh superinfection. Conversely, early CC surgical management could cause mesh displacement and lead to CDH recurrence, requiring reintervention. We present the rare case of a CC occurring in a neonate with a prenatally diagnosed right CDH. One month after an uncomplicated CDH repair with mesh, while the patient was still hospitalized for pulmonary hypertension, she developed progressive cholestasis and acholic stools. Investigations revealed a nonpreviously suspected CC. Conservative treatment was attempted, but CC perforation with secondary biliary peritonitis occurred. Open CC excision with a Roux-en-Y hepaticojejunostomy was therefore performed on day of life (DOL) 41. Having suffered no short-term surgical complications, the patient was discharged on DOL 83 because of prolonged ventilatory support due to pulmonary hypertension. Now 12 months after surgery, she is doing well with normal liver function tests and imaging studies. In summary, CC should be considered in the differential diagnosis of progressive cholestasis in patients with CDH. Surgical repair of a symptomatic CC should not be delayed even in the presence of mesh given the risks of CC complications.</p>\",\"PeriodicalId\":43204,\"journal\":{\"name\":\"European Journal of Pediatric Surgery Reports\",\"volume\":\"12 1\",\"pages\":\"e68-e72\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-10-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11518628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pediatric Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0044-1791813\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1791813","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
先天性膈疝(CDH)患者可能伴有其他先天性畸形,但伴有胆总管囊肿(CC)的病例却很少见。同时诊断出这两种畸形会使患者的治疗变得复杂。关于切除 CC 的理想时机,目前还没有达成共识。未修复的CC有发展成胆汁淤积、胆总管结石和胆管炎的风险。在使用网片进行CDH修复后,延迟CC修复引起的继发性细菌易位可能导致网片超级感染。反之,过早进行CC手术治疗可能会导致网片移位,导致CDH复发,需要重新进行手术治疗。我们介绍了一例产前确诊为右侧 CDH 的新生儿发生 CC 的罕见病例。在使用网片进行无并发症的CDH修补术一个月后,患者因肺动脉高压仍在住院治疗,但出现了进行性胆汁淤积和大便隐痛。检查结果显示她患有之前未被怀疑的CC。医生尝试了保守治疗,但还是发生了CC穿孔和继发性胆道腹膜炎。因此,患者在生命第41天(DOL)进行了开放式CC切除术和Roux-en-Y肝空肠吻合术。患者没有出现短期手术并发症,但由于肺动脉高压而需要长时间的呼吸支持,因此于第 83 天出院。术后 12 个月,她的肝功能检查和影像学检查均正常。总之,CDH 患者进行性胆汁淤积的鉴别诊断中应考虑到 CC。鉴于CC并发症的风险,即使存在网片,也不应延迟对有症状的CC进行手术修复。
Choledochal Cyst and Right Congenital Diaphragmatic Hernia: When to Intervene?
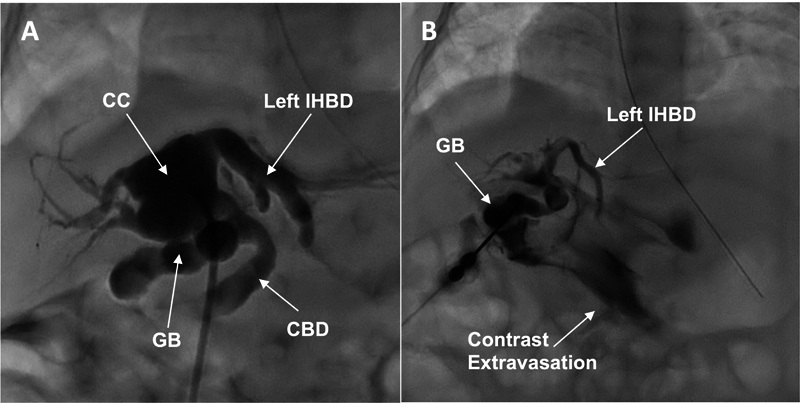
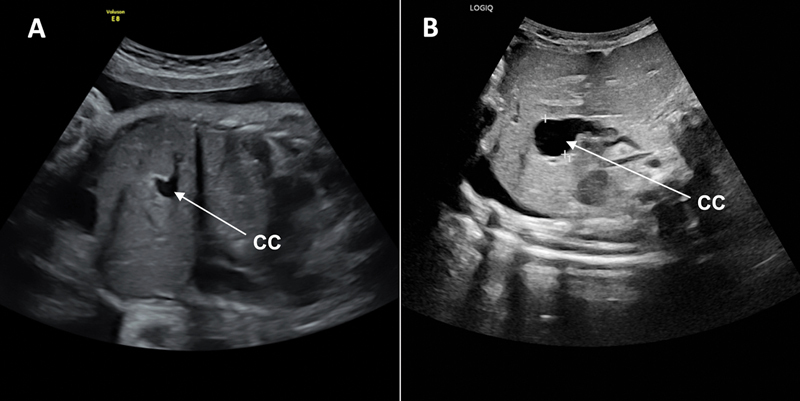
Patients with congenital diaphragmatic hernia (CDH) can present with other congenital anomalies, but an associated choledochal cyst (CC) has rarely been described. The simultaneous diagnosis of both anomalies complicates patient management. There is no consensus on the ideal timing for CC excision. Unrepaired CC is associated with risks of developing biliary sludge, choledocholithiasis, and cholangitis. After a CDH repair with mesh, secondary bacterial translocation caused by a delayed CC repair could lead to mesh superinfection. Conversely, early CC surgical management could cause mesh displacement and lead to CDH recurrence, requiring reintervention. We present the rare case of a CC occurring in a neonate with a prenatally diagnosed right CDH. One month after an uncomplicated CDH repair with mesh, while the patient was still hospitalized for pulmonary hypertension, she developed progressive cholestasis and acholic stools. Investigations revealed a nonpreviously suspected CC. Conservative treatment was attempted, but CC perforation with secondary biliary peritonitis occurred. Open CC excision with a Roux-en-Y hepaticojejunostomy was therefore performed on day of life (DOL) 41. Having suffered no short-term surgical complications, the patient was discharged on DOL 83 because of prolonged ventilatory support due to pulmonary hypertension. Now 12 months after surgery, she is doing well with normal liver function tests and imaging studies. In summary, CC should be considered in the differential diagnosis of progressive cholestasis in patients with CDH. Surgical repair of a symptomatic CC should not be delayed even in the presence of mesh given the risks of CC complications.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
