{"title":"估算 Pao2/Fio2 比率的连续无创方法","authors":"Francis-Olivier Beauchamp, Michaël Sauthier","doi":"10.1097/CCE.0000000000001174","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To validate a method for continuously estimating the Pao<sub>2</sub>/Fio<sub>2</sub> (PF) ratio in all critically ill pediatric patients using only standard continuous data monitoring.</p><p><strong>Design: </strong>Retrospective study on a high temporal resolution database.</p><p><strong>Setting: </strong>PICU in Montreal, QC, Canada.</p><p><strong>Patients/subjects: </strong>We included any patients admitted from May 2015 to May 2023 who had an arterial blood gas (ABG) with concurrent continuous pulsed oximetry saturation (Spo<sub>2</sub>) values. We used our previously validated mathematical model to determine the magnitude of hypoxemia by computing the estimated ePao<sub>2</sub>/Fio<sub>2</sub> (ePF) ratio and comparing it to the Spo<sub>2</sub>/Fio<sub>2</sub> (SF), using PF ratio as the reference standard.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We analyzed a total of 20,828 ABGs. When Spo<sub>2</sub> was below or equal to 97%, the ePF ratio showed a significantly better hypoxemia classification (none, light/moderate, or severe) than the SF ratio (0.80 vs. 0.72; <i>p</i> < 0.001), a lower fixed bias (16.26 vs. -35.24; <i>p</i> < 0.001), a lower mean absolute error (37.92 vs. 63.93; <i>p</i> < 0.001) and a lower proportional bias (slope of 1.01 vs. 0.81; <i>p</i> < 0.001). ePF ratio has also a better limits of agreement difference from Bland-Altman plot (248.10 vs. 292.45; <i>p</i> < 0.001) and coefficient of determination (0.68 vs. 0.59; <i>p</i> < 0.001). When Spo<sub>2</sub> was above 97%, the ePF ratio had better classification with Kappa (0.53 vs. 0.43; <i>p</i> < 0.001) and lower fixed bias (-0.63 vs. 65.68; <i>p</i> < 0.001).</p><p><strong>Conclusions: </strong>The PF ratio based on ePF allows for a continuous estimation of hypoxemia severity with a better performance than the SF ratio.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 11","pages":"e1174"},"PeriodicalIF":2.7000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11519398/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Continuous and Noninvasive Method to Estimate Pao<sub>2</sub>/Fio<sub>2</sub> Ratio.\",\"authors\":\"Francis-Olivier Beauchamp, Michaël Sauthier\",\"doi\":\"10.1097/CCE.0000000000001174\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To validate a method for continuously estimating the Pao<sub>2</sub>/Fio<sub>2</sub> (PF) ratio in all critically ill pediatric patients using only standard continuous data monitoring.</p><p><strong>Design: </strong>Retrospective study on a high temporal resolution database.</p><p><strong>Setting: </strong>PICU in Montreal, QC, Canada.</p><p><strong>Patients/subjects: </strong>We included any patients admitted from May 2015 to May 2023 who had an arterial blood gas (ABG) with concurrent continuous pulsed oximetry saturation (Spo<sub>2</sub>) values. We used our previously validated mathematical model to determine the magnitude of hypoxemia by computing the estimated ePao<sub>2</sub>/Fio<sub>2</sub> (ePF) ratio and comparing it to the Spo<sub>2</sub>/Fio<sub>2</sub> (SF), using PF ratio as the reference standard.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We analyzed a total of 20,828 ABGs. When Spo<sub>2</sub> was below or equal to 97%, the ePF ratio showed a significantly better hypoxemia classification (none, light/moderate, or severe) than the SF ratio (0.80 vs. 0.72; <i>p</i> < 0.001), a lower fixed bias (16.26 vs. -35.24; <i>p</i> < 0.001), a lower mean absolute error (37.92 vs. 63.93; <i>p</i> < 0.001) and a lower proportional bias (slope of 1.01 vs. 0.81; <i>p</i> < 0.001). ePF ratio has also a better limits of agreement difference from Bland-Altman plot (248.10 vs. 292.45; <i>p</i> < 0.001) and coefficient of determination (0.68 vs. 0.59; <i>p</i> < 0.001). When Spo<sub>2</sub> was above 97%, the ePF ratio had better classification with Kappa (0.53 vs. 0.43; <i>p</i> < 0.001) and lower fixed bias (-0.63 vs. 65.68; <i>p</i> < 0.001).</p><p><strong>Conclusions: </strong>The PF ratio based on ePF allows for a continuous estimation of hypoxemia severity with a better performance than the SF ratio.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"6 11\",\"pages\":\"e1174\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11519398/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001174\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001174","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
目的验证一种仅使用标准连续数据监测对所有重症儿科患者的 Pao2/Fio2 (PF) 比率进行连续估算的方法:设计:对高时间分辨率数据库进行回顾性研究:患者/受试者:我们纳入了从 2015 年 5 月至 2023 年 5 月期间入院的所有患者,这些患者均有动脉血气 (ABG) 和同期连续脉冲血氧饱和度 (Spo2) 值。我们使用之前验证过的数学模型,通过计算估计的 ePao2/Fio2 (ePF) 比值来确定低氧血症的程度,并将其与 Spo2/Fio2 (SF) 进行比较,以 PF 比值作为参考标准:干预措施:无:我们共分析了 20,828 份 ABG。当 Spo2 低于或等于 97% 时,ePF 比值显示的低氧血症分类(无、轻度/中度或重度)明显优于 SF 比值(0.80 vs. 0.72;p <0.001),固定偏差更低(16.26 vs. -35.24;p <0.001),平均绝对误差更低(37.从布兰德-阿尔特曼图(248.10 vs. 292.45; p < 0.001)和决定系数(0.68 vs. 0.59; p < 0.001)来看,ePF 比值也具有更好的一致性差异(248.10 vs. 292.45; p < 0.001)和决定系数(0.68 vs. 0.59; p < 0.001)。当 Spo2 超过 97% 时,ePF 比率的分类效果更好,Kappa 值(0.53 vs. 0.43;p < 0.001)和固定偏差(-0.63 vs. 65.68;p < 0.001)更低:结论:基于 ePF 的 PF 比值可连续估计低氧血症的严重程度,其性能优于 SF 比值。
A Continuous and Noninvasive Method to Estimate Pao2/Fio2 Ratio.
Objectives: To validate a method for continuously estimating the Pao2/Fio2 (PF) ratio in all critically ill pediatric patients using only standard continuous data monitoring.
Design: Retrospective study on a high temporal resolution database.
Setting: PICU in Montreal, QC, Canada.
Patients/subjects: We included any patients admitted from May 2015 to May 2023 who had an arterial blood gas (ABG) with concurrent continuous pulsed oximetry saturation (Spo2) values. We used our previously validated mathematical model to determine the magnitude of hypoxemia by computing the estimated ePao2/Fio2 (ePF) ratio and comparing it to the Spo2/Fio2 (SF), using PF ratio as the reference standard.
Interventions: None.
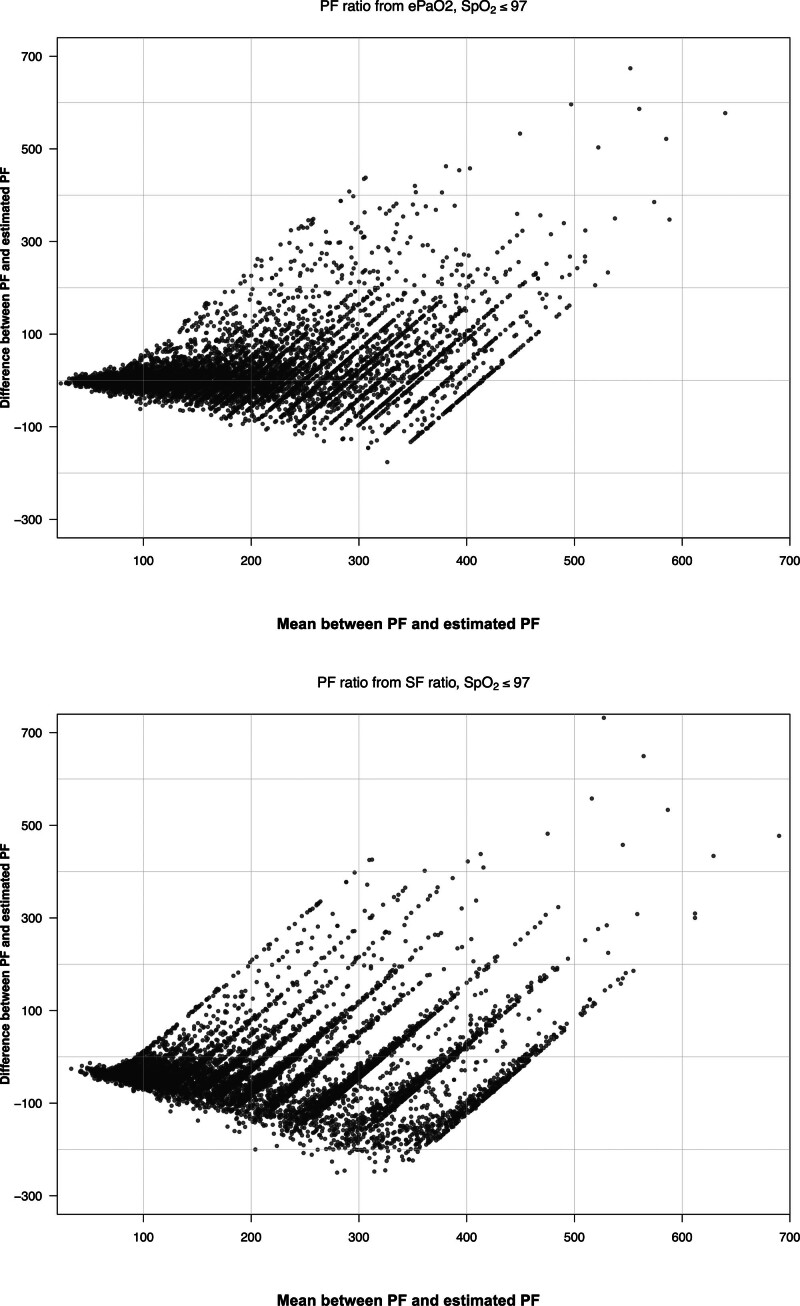
Measurements and main results: We analyzed a total of 20,828 ABGs. When Spo2 was below or equal to 97%, the ePF ratio showed a significantly better hypoxemia classification (none, light/moderate, or severe) than the SF ratio (0.80 vs. 0.72; p < 0.001), a lower fixed bias (16.26 vs. -35.24; p < 0.001), a lower mean absolute error (37.92 vs. 63.93; p < 0.001) and a lower proportional bias (slope of 1.01 vs. 0.81; p < 0.001). ePF ratio has also a better limits of agreement difference from Bland-Altman plot (248.10 vs. 292.45; p < 0.001) and coefficient of determination (0.68 vs. 0.59; p < 0.001). When Spo2 was above 97%, the ePF ratio had better classification with Kappa (0.53 vs. 0.43; p < 0.001) and lower fixed bias (-0.63 vs. 65.68; p < 0.001).
Conclusions: The PF ratio based on ePF allows for a continuous estimation of hypoxemia severity with a better performance than the SF ratio.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
