Patrizio Lancellotti, Tadafumi Sugimoto, Magnus Bäck
{"title":"重新审视继发性二尖瓣反流阈值的严重程度:RESHAPE-HF2 试验的启示和教训。","authors":"Patrizio Lancellotti, Tadafumi Sugimoto, Magnus Bäck","doi":"10.1093/ehjopen/oeae084","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>This article revisits the severity threshold for secondary mitral regurgitation (MR), focusing on insights and lessons from the RESHAPE-HF2 trial. It aims to challenge the traditional effective regurgitant orifice area (EROA) threshold of ≥0.40 cm<sup>2</sup> used for intervention, suggesting that earlier intervention may benefit patients with lower EROA. It also explores how transcatheter edge-to-edge repair (TEER) improves outcomes in patients with secondary MR and assesses the impact of left ventricular (LV) remodeling on treatment success.</p><p><strong>Methods and results: </strong>The RESHAPE-HF2 trial evaluated the use of TEER in patients with moderate-to-severe secondary MR, comparing outcomes in those with an EROA ≥0.2 cm<sup>2</sup> and no extensive LV remodeling. TEER significantly reduced heart failure hospitalizations and improved quality of life in these patients. This supports the notion that patients with less severe MR, who still show symptoms despite optimal medical therapy, may benefit from earlier intervention. Comparisons with COAPT and MITRA-FR trials underscored the importance of selecting patients based on MR severity relative to LV dilatation.</p><p><strong>Conclusions: </strong>The RESHAPE-HF2 trial highlights the need to reconsider the current EROA threshold for secondary MR intervention. TEER has shown to be beneficial even in patients with lower MR severity, suggesting that earlier intervention could improve outcomes. A more dynamic and integrated approach, considering both MR severity and LV remodeling, is essential for optimizing patient selection and treatment success.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 5","pages":"oeae084"},"PeriodicalIF":4.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520926/pdf/","citationCount":"0","resultStr":"{\"title\":\"Revisiting secondary mitral regurgitation threshold severity: insights and lessons from the RESHAPE-HF2 trial.\",\"authors\":\"Patrizio Lancellotti, Tadafumi Sugimoto, Magnus Bäck\",\"doi\":\"10.1093/ehjopen/oeae084\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>This article revisits the severity threshold for secondary mitral regurgitation (MR), focusing on insights and lessons from the RESHAPE-HF2 trial. It aims to challenge the traditional effective regurgitant orifice area (EROA) threshold of ≥0.40 cm<sup>2</sup> used for intervention, suggesting that earlier intervention may benefit patients with lower EROA. It also explores how transcatheter edge-to-edge repair (TEER) improves outcomes in patients with secondary MR and assesses the impact of left ventricular (LV) remodeling on treatment success.</p><p><strong>Methods and results: </strong>The RESHAPE-HF2 trial evaluated the use of TEER in patients with moderate-to-severe secondary MR, comparing outcomes in those with an EROA ≥0.2 cm<sup>2</sup> and no extensive LV remodeling. TEER significantly reduced heart failure hospitalizations and improved quality of life in these patients. This supports the notion that patients with less severe MR, who still show symptoms despite optimal medical therapy, may benefit from earlier intervention. Comparisons with COAPT and MITRA-FR trials underscored the importance of selecting patients based on MR severity relative to LV dilatation.</p><p><strong>Conclusions: </strong>The RESHAPE-HF2 trial highlights the need to reconsider the current EROA threshold for secondary MR intervention. TEER has shown to be beneficial even in patients with lower MR severity, suggesting that earlier intervention could improve outcomes. A more dynamic and integrated approach, considering both MR severity and LV remodeling, is essential for optimizing patient selection and treatment success.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"4 5\",\"pages\":\"oeae084\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520926/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeae084\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae084","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Revisiting secondary mitral regurgitation threshold severity: insights and lessons from the RESHAPE-HF2 trial.
Aims: This article revisits the severity threshold for secondary mitral regurgitation (MR), focusing on insights and lessons from the RESHAPE-HF2 trial. It aims to challenge the traditional effective regurgitant orifice area (EROA) threshold of ≥0.40 cm2 used for intervention, suggesting that earlier intervention may benefit patients with lower EROA. It also explores how transcatheter edge-to-edge repair (TEER) improves outcomes in patients with secondary MR and assesses the impact of left ventricular (LV) remodeling on treatment success.
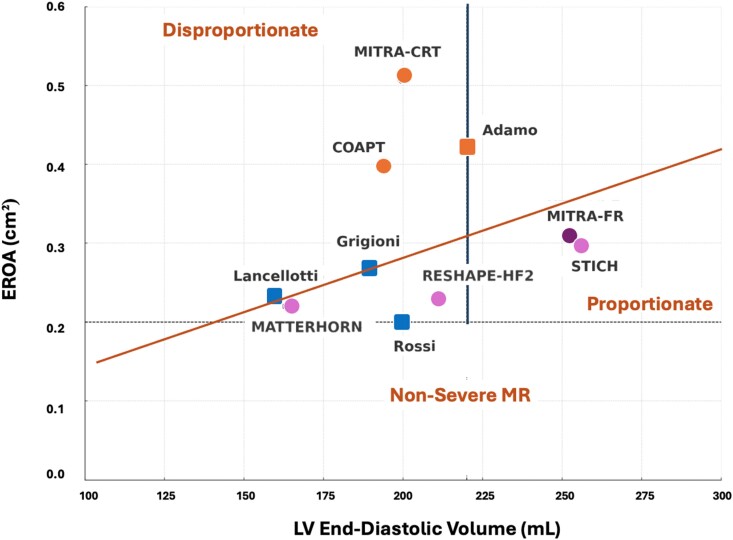
Methods and results: The RESHAPE-HF2 trial evaluated the use of TEER in patients with moderate-to-severe secondary MR, comparing outcomes in those with an EROA ≥0.2 cm2 and no extensive LV remodeling. TEER significantly reduced heart failure hospitalizations and improved quality of life in these patients. This supports the notion that patients with less severe MR, who still show symptoms despite optimal medical therapy, may benefit from earlier intervention. Comparisons with COAPT and MITRA-FR trials underscored the importance of selecting patients based on MR severity relative to LV dilatation.
Conclusions: The RESHAPE-HF2 trial highlights the need to reconsider the current EROA threshold for secondary MR intervention. TEER has shown to be beneficial even in patients with lower MR severity, suggesting that earlier intervention could improve outcomes. A more dynamic and integrated approach, considering both MR severity and LV remodeling, is essential for optimizing patient selection and treatment success.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
