{"title":"药物再利用:硼替佐米治疗PTEN缺陷的iCCA","authors":"Shi-jia Dai, Tian-yi Jiang, Zhen-gang Yuan","doi":"10.1002/ctd2.70004","DOIUrl":null,"url":null,"abstract":"<p>Intrahepatic cholangiocarcinoma (iCCA) is an epithelial malignancy arising from intrahepatic biliary tract, characterised by a dismal prognosis with limited therapeutic alternatives.<span><sup>1</sup></span> The standard first-line treatment for patients with unresectable iCCA includes gemcitabine-based chemotherapy and immunotherapy. However, the objective response rate (ORR) of first-line treatment is below 30%, and there is currently insufficient evidence to support the use of second-line chemotherapy.<span><sup>2, 3</sup></span> This underscores an urgent need to identify novel therapeutic targets and effective drugs for iCCA.</p><p>Our previous research has demonstrated that phosphatase and tension homolog (PTEN), a tumour suppressor which counteracts phosphatidylinositol 3-kinase (PI3K)–AKT signalling, is frequently mutated or deleted in iCCA.<span><sup>4</sup></span> We established a spontaneous iCCA model in mice through liver-specific PTEN disruption and Kras activation, highlighting the crucial role of PTEN in iCCA tumourigenesis.<span><sup>5</sup></span> Importantly, we identified PTEN as a pivotal regulator of both the lysosomal and proteasomal systems, which are essential for maintaining cellular proteostasis in CCA cells. PTEN drives lysosome biogenesis and acidification through its protein phosphatase activity, which dephosphorylates transcription factor EB (TFEB) at Ser211, thereby regulating exosome secretion and iCCA metastasis.<span><sup>6</sup></span> Simultaneously, PTEN inhibits proteasomal transcription via its lipid phosphatase activity in a BACH1/MAFF-dependent manner.<span><sup>7</sup></span> Consequently, PTEN deficiency enhances protein synthesis and proteasomal activity, creating a dependency on the proteasome for iCCA cell growth and survival. Therefore, targeting the proteasome machinery by inhibitor bortezomib induces more apoptosis in PTEN-deficient iCCA cells.</p><p>We subsequently conducted a clinical trial (NCT03345303) to assess whether PTEN-deficient iCCA patients could benefit from bortezomib treatment after failure of first-line chemotherapy, investigating PTEN as a potential biomarker for proteasome inhibition. This open-label, single-arm, phase II clinical trial was conducted at the Eastern Hepatobiliary Surgery Hospital, Shanghai. A total of 130 advanced iCCA patients were screened for PTEN expression and 16 were enrolled and treated with single-agent bortezomib. Among the intent-to-treat cohort (<i>n</i> = 16), the ORR was 18.75% (three out of 16), and the disease control rate (DCR) was 43.75% (seven out of 16). Notably, three patients did not undergo efficacy assessment, resulting in more favourable outcomes in the per-protocol (PP) cohort (<i>n</i> = 13), which demonstrated an ORR of 23.08% and a DCR of 53.85%. The median progression-free survival (PFS) was 3.6 months, and median overall survival (OS) was 9.6 months in the PP cohort. To our knowledge, the primary efficacy endpoint of our trail, the ORR in the PP cohort, is only lower than previous reports on FGFR inhibitors, but significantly improved compared with other second-line treatment regimens, such as FOLFOX (5%), regorafenib (11%) and levatinib in combination with pabolizumab (10%). Additionally, bortezomib-related toxicities were deemed acceptable, with no treatment-related deaths and platelet count decrease being the most common adverse effect. These results indicate that bortezomib is a promising second-line therapy for PTEN-deficient iCCA.<span><sup>8</sup></span></p><p>Building on the insights gained from our second-line monotherapy study, we are advancing to a phase II interventional clinical trial (ChiCTR2000035916) designed to further evaluate the efficacy of gemcitabine-based chemotherapy in combination with bortezomib for treating cholangiocarcinoma (CCA) (see Figure 1). This trial aims to enrol 200 patients with advanced CCA and will explore whether alterations in PTEN and PIK3CA/B influence the effectiveness of this combined therapy, with the ultimate objective of developing a molecularly tailored treatment regimen for CCA in China. Preliminary findings suggest that patients with PTEN deficiency derive greater benefit from this combined therapy, corroborating the results observed in our second-line monotherapy study.</p><p>To date, the United States Food and Drug Administration has approved three proteasome inhibitors for the treatment of multiple myeloma: bortezomib, carfilzomib and ixazomib.<span><sup>9</sup></span> However, the application of proteasome inhibitors in solid tumours remains limited. In this study, we focus on bortezomib. As a first-generation proteasome inhibitor, bortezomib has been in clinical use for nearly 20 years,<span><sup>10</sup></span> with extensive research on its safety, tolerability and pharmacokinetic properties, making it more amenable to ‘drug repositioning’. Notably, a prior phase II trial assessing bortezomib's therapeutic efficacy in unselected biliary tract cancer (BTC) patients failed to meet its primary endpoint but achieved encouraging disease stability and median PFS. This suggests that biomarker-driven patient selection and drug combination strategies may offer significant benefits. Our previous research revealed PTEN-deficient iCCA cells displayed high proteasome activity and proliferation, which created susceptibility to bortezomib both in vitro and in vivo. Mechanistically, we identified the PTEN–AKT–FOXO1–BACH1/MAFF signalling pathway as regulating the transcription of proteasome genes and influencing the sensitivity of bortezomib. Consequently, we have initiated a prospective clinical trial, unprecedentedly evaluating the proteasome inhibitor bortezomib in a selected ICC cohort with PTEN deficiency and obtained an improved therapeutic outcome.</p><p>The prompt identification of PTEN-deficient CCA patients is crucial due to the aggressive nature and rapid progression of tumours in these individuals. Effective and timely screening is essential for guiding subsequent second-line treatments. In this study, we utilised multiple techniques to evaluate PTEN deficiency, including immunohistochemistry (IHC), next-generation sequencing (NGS) and RNA scope technology.<span><sup>8</sup></span> Our findings revealed a strong correlation between PTEN protein expression and genetic alterations. Consistent with our previous research, which involved IHC and gene sequencing of PTEN in 50 ICC patients, PTEN deficiency was significantly associated with genetic alterations. PTEN homozygous deletions or frameshift mutations typically result in absent protein expression; thus, we advocate for IHC as the initial screening method. When sample availability allows, both IHC and NGS should be conducted to ensure comprehensive assessment.</p><p>Additionally, analysis of the Genomics of Drug Sensitivity in Cancer and the Cancer Therapeutics Response Portal databases revealed that PTEN loss enhances the sensitivity of proteasome inhibitors across various tumours, indicating that our findings may have broad applicability.<span><sup>7</sup></span> Similar cellular and animal phenotypes have been observed in gallbladder cancer<span><sup>4</sup></span> and glioblastoma,<span><sup>11</sup></span> suggesting that precision therapeutic approaches based on PTEN molecular subtyping with proteasome inhibitors may be extended to other tumours, benefiting more patients with PTEN deficiency.</p><p>In summary, our research demonstrates that bortezomib shows promising efficacy with manageable toxicity as a second-line therapy for PTEN-deficient iCCA, with manageable toxicity and a median OS of 9.6 months in the PP cohort. These results support the broaden application of proteasome inhibitors in solid tumours and provide renewed hope for patients with PTEN-deficient malignancies.</p>","PeriodicalId":72605,"journal":{"name":"Clinical and translational discovery","volume":"4 6","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctd2.70004","citationCount":"0","resultStr":"{\"title\":\"Drug repurposing: Bortezomib in the treatment of PTEN-deficient iCCA\",\"authors\":\"Shi-jia Dai, Tian-yi Jiang, Zhen-gang Yuan\",\"doi\":\"10.1002/ctd2.70004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Intrahepatic cholangiocarcinoma (iCCA) is an epithelial malignancy arising from intrahepatic biliary tract, characterised by a dismal prognosis with limited therapeutic alternatives.<span><sup>1</sup></span> The standard first-line treatment for patients with unresectable iCCA includes gemcitabine-based chemotherapy and immunotherapy. However, the objective response rate (ORR) of first-line treatment is below 30%, and there is currently insufficient evidence to support the use of second-line chemotherapy.<span><sup>2, 3</sup></span> This underscores an urgent need to identify novel therapeutic targets and effective drugs for iCCA.</p><p>Our previous research has demonstrated that phosphatase and tension homolog (PTEN), a tumour suppressor which counteracts phosphatidylinositol 3-kinase (PI3K)–AKT signalling, is frequently mutated or deleted in iCCA.<span><sup>4</sup></span> We established a spontaneous iCCA model in mice through liver-specific PTEN disruption and Kras activation, highlighting the crucial role of PTEN in iCCA tumourigenesis.<span><sup>5</sup></span> Importantly, we identified PTEN as a pivotal regulator of both the lysosomal and proteasomal systems, which are essential for maintaining cellular proteostasis in CCA cells. PTEN drives lysosome biogenesis and acidification through its protein phosphatase activity, which dephosphorylates transcription factor EB (TFEB) at Ser211, thereby regulating exosome secretion and iCCA metastasis.<span><sup>6</sup></span> Simultaneously, PTEN inhibits proteasomal transcription via its lipid phosphatase activity in a BACH1/MAFF-dependent manner.<span><sup>7</sup></span> Consequently, PTEN deficiency enhances protein synthesis and proteasomal activity, creating a dependency on the proteasome for iCCA cell growth and survival. Therefore, targeting the proteasome machinery by inhibitor bortezomib induces more apoptosis in PTEN-deficient iCCA cells.</p><p>We subsequently conducted a clinical trial (NCT03345303) to assess whether PTEN-deficient iCCA patients could benefit from bortezomib treatment after failure of first-line chemotherapy, investigating PTEN as a potential biomarker for proteasome inhibition. This open-label, single-arm, phase II clinical trial was conducted at the Eastern Hepatobiliary Surgery Hospital, Shanghai. A total of 130 advanced iCCA patients were screened for PTEN expression and 16 were enrolled and treated with single-agent bortezomib. Among the intent-to-treat cohort (<i>n</i> = 16), the ORR was 18.75% (three out of 16), and the disease control rate (DCR) was 43.75% (seven out of 16). Notably, three patients did not undergo efficacy assessment, resulting in more favourable outcomes in the per-protocol (PP) cohort (<i>n</i> = 13), which demonstrated an ORR of 23.08% and a DCR of 53.85%. The median progression-free survival (PFS) was 3.6 months, and median overall survival (OS) was 9.6 months in the PP cohort. To our knowledge, the primary efficacy endpoint of our trail, the ORR in the PP cohort, is only lower than previous reports on FGFR inhibitors, but significantly improved compared with other second-line treatment regimens, such as FOLFOX (5%), regorafenib (11%) and levatinib in combination with pabolizumab (10%). Additionally, bortezomib-related toxicities were deemed acceptable, with no treatment-related deaths and platelet count decrease being the most common adverse effect. These results indicate that bortezomib is a promising second-line therapy for PTEN-deficient iCCA.<span><sup>8</sup></span></p><p>Building on the insights gained from our second-line monotherapy study, we are advancing to a phase II interventional clinical trial (ChiCTR2000035916) designed to further evaluate the efficacy of gemcitabine-based chemotherapy in combination with bortezomib for treating cholangiocarcinoma (CCA) (see Figure 1). This trial aims to enrol 200 patients with advanced CCA and will explore whether alterations in PTEN and PIK3CA/B influence the effectiveness of this combined therapy, with the ultimate objective of developing a molecularly tailored treatment regimen for CCA in China. Preliminary findings suggest that patients with PTEN deficiency derive greater benefit from this combined therapy, corroborating the results observed in our second-line monotherapy study.</p><p>To date, the United States Food and Drug Administration has approved three proteasome inhibitors for the treatment of multiple myeloma: bortezomib, carfilzomib and ixazomib.<span><sup>9</sup></span> However, the application of proteasome inhibitors in solid tumours remains limited. In this study, we focus on bortezomib. As a first-generation proteasome inhibitor, bortezomib has been in clinical use for nearly 20 years,<span><sup>10</sup></span> with extensive research on its safety, tolerability and pharmacokinetic properties, making it more amenable to ‘drug repositioning’. Notably, a prior phase II trial assessing bortezomib's therapeutic efficacy in unselected biliary tract cancer (BTC) patients failed to meet its primary endpoint but achieved encouraging disease stability and median PFS. This suggests that biomarker-driven patient selection and drug combination strategies may offer significant benefits. Our previous research revealed PTEN-deficient iCCA cells displayed high proteasome activity and proliferation, which created susceptibility to bortezomib both in vitro and in vivo. Mechanistically, we identified the PTEN–AKT–FOXO1–BACH1/MAFF signalling pathway as regulating the transcription of proteasome genes and influencing the sensitivity of bortezomib. Consequently, we have initiated a prospective clinical trial, unprecedentedly evaluating the proteasome inhibitor bortezomib in a selected ICC cohort with PTEN deficiency and obtained an improved therapeutic outcome.</p><p>The prompt identification of PTEN-deficient CCA patients is crucial due to the aggressive nature and rapid progression of tumours in these individuals. Effective and timely screening is essential for guiding subsequent second-line treatments. In this study, we utilised multiple techniques to evaluate PTEN deficiency, including immunohistochemistry (IHC), next-generation sequencing (NGS) and RNA scope technology.<span><sup>8</sup></span> Our findings revealed a strong correlation between PTEN protein expression and genetic alterations. Consistent with our previous research, which involved IHC and gene sequencing of PTEN in 50 ICC patients, PTEN deficiency was significantly associated with genetic alterations. PTEN homozygous deletions or frameshift mutations typically result in absent protein expression; thus, we advocate for IHC as the initial screening method. When sample availability allows, both IHC and NGS should be conducted to ensure comprehensive assessment.</p><p>Additionally, analysis of the Genomics of Drug Sensitivity in Cancer and the Cancer Therapeutics Response Portal databases revealed that PTEN loss enhances the sensitivity of proteasome inhibitors across various tumours, indicating that our findings may have broad applicability.<span><sup>7</sup></span> Similar cellular and animal phenotypes have been observed in gallbladder cancer<span><sup>4</sup></span> and glioblastoma,<span><sup>11</sup></span> suggesting that precision therapeutic approaches based on PTEN molecular subtyping with proteasome inhibitors may be extended to other tumours, benefiting more patients with PTEN deficiency.</p><p>In summary, our research demonstrates that bortezomib shows promising efficacy with manageable toxicity as a second-line therapy for PTEN-deficient iCCA, with manageable toxicity and a median OS of 9.6 months in the PP cohort. These results support the broaden application of proteasome inhibitors in solid tumours and provide renewed hope for patients with PTEN-deficient malignancies.</p>\",\"PeriodicalId\":72605,\"journal\":{\"name\":\"Clinical and translational discovery\",\"volume\":\"4 6\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-10-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctd2.70004\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and translational discovery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ctd2.70004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and translational discovery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctd2.70004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Drug repurposing: Bortezomib in the treatment of PTEN-deficient iCCA
Intrahepatic cholangiocarcinoma (iCCA) is an epithelial malignancy arising from intrahepatic biliary tract, characterised by a dismal prognosis with limited therapeutic alternatives.1 The standard first-line treatment for patients with unresectable iCCA includes gemcitabine-based chemotherapy and immunotherapy. However, the objective response rate (ORR) of first-line treatment is below 30%, and there is currently insufficient evidence to support the use of second-line chemotherapy.2, 3 This underscores an urgent need to identify novel therapeutic targets and effective drugs for iCCA.
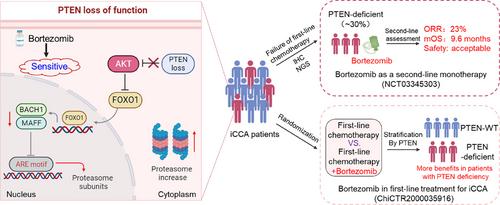
Our previous research has demonstrated that phosphatase and tension homolog (PTEN), a tumour suppressor which counteracts phosphatidylinositol 3-kinase (PI3K)–AKT signalling, is frequently mutated or deleted in iCCA.4 We established a spontaneous iCCA model in mice through liver-specific PTEN disruption and Kras activation, highlighting the crucial role of PTEN in iCCA tumourigenesis.5 Importantly, we identified PTEN as a pivotal regulator of both the lysosomal and proteasomal systems, which are essential for maintaining cellular proteostasis in CCA cells. PTEN drives lysosome biogenesis and acidification through its protein phosphatase activity, which dephosphorylates transcription factor EB (TFEB) at Ser211, thereby regulating exosome secretion and iCCA metastasis.6 Simultaneously, PTEN inhibits proteasomal transcription via its lipid phosphatase activity in a BACH1/MAFF-dependent manner.7 Consequently, PTEN deficiency enhances protein synthesis and proteasomal activity, creating a dependency on the proteasome for iCCA cell growth and survival. Therefore, targeting the proteasome machinery by inhibitor bortezomib induces more apoptosis in PTEN-deficient iCCA cells.
We subsequently conducted a clinical trial (NCT03345303) to assess whether PTEN-deficient iCCA patients could benefit from bortezomib treatment after failure of first-line chemotherapy, investigating PTEN as a potential biomarker for proteasome inhibition. This open-label, single-arm, phase II clinical trial was conducted at the Eastern Hepatobiliary Surgery Hospital, Shanghai. A total of 130 advanced iCCA patients were screened for PTEN expression and 16 were enrolled and treated with single-agent bortezomib. Among the intent-to-treat cohort (n = 16), the ORR was 18.75% (three out of 16), and the disease control rate (DCR) was 43.75% (seven out of 16). Notably, three patients did not undergo efficacy assessment, resulting in more favourable outcomes in the per-protocol (PP) cohort (n = 13), which demonstrated an ORR of 23.08% and a DCR of 53.85%. The median progression-free survival (PFS) was 3.6 months, and median overall survival (OS) was 9.6 months in the PP cohort. To our knowledge, the primary efficacy endpoint of our trail, the ORR in the PP cohort, is only lower than previous reports on FGFR inhibitors, but significantly improved compared with other second-line treatment regimens, such as FOLFOX (5%), regorafenib (11%) and levatinib in combination with pabolizumab (10%). Additionally, bortezomib-related toxicities were deemed acceptable, with no treatment-related deaths and platelet count decrease being the most common adverse effect. These results indicate that bortezomib is a promising second-line therapy for PTEN-deficient iCCA.8
Building on the insights gained from our second-line monotherapy study, we are advancing to a phase II interventional clinical trial (ChiCTR2000035916) designed to further evaluate the efficacy of gemcitabine-based chemotherapy in combination with bortezomib for treating cholangiocarcinoma (CCA) (see Figure 1). This trial aims to enrol 200 patients with advanced CCA and will explore whether alterations in PTEN and PIK3CA/B influence the effectiveness of this combined therapy, with the ultimate objective of developing a molecularly tailored treatment regimen for CCA in China. Preliminary findings suggest that patients with PTEN deficiency derive greater benefit from this combined therapy, corroborating the results observed in our second-line monotherapy study.
To date, the United States Food and Drug Administration has approved three proteasome inhibitors for the treatment of multiple myeloma: bortezomib, carfilzomib and ixazomib.9 However, the application of proteasome inhibitors in solid tumours remains limited. In this study, we focus on bortezomib. As a first-generation proteasome inhibitor, bortezomib has been in clinical use for nearly 20 years,10 with extensive research on its safety, tolerability and pharmacokinetic properties, making it more amenable to ‘drug repositioning’. Notably, a prior phase II trial assessing bortezomib's therapeutic efficacy in unselected biliary tract cancer (BTC) patients failed to meet its primary endpoint but achieved encouraging disease stability and median PFS. This suggests that biomarker-driven patient selection and drug combination strategies may offer significant benefits. Our previous research revealed PTEN-deficient iCCA cells displayed high proteasome activity and proliferation, which created susceptibility to bortezomib both in vitro and in vivo. Mechanistically, we identified the PTEN–AKT–FOXO1–BACH1/MAFF signalling pathway as regulating the transcription of proteasome genes and influencing the sensitivity of bortezomib. Consequently, we have initiated a prospective clinical trial, unprecedentedly evaluating the proteasome inhibitor bortezomib in a selected ICC cohort with PTEN deficiency and obtained an improved therapeutic outcome.
The prompt identification of PTEN-deficient CCA patients is crucial due to the aggressive nature and rapid progression of tumours in these individuals. Effective and timely screening is essential for guiding subsequent second-line treatments. In this study, we utilised multiple techniques to evaluate PTEN deficiency, including immunohistochemistry (IHC), next-generation sequencing (NGS) and RNA scope technology.8 Our findings revealed a strong correlation between PTEN protein expression and genetic alterations. Consistent with our previous research, which involved IHC and gene sequencing of PTEN in 50 ICC patients, PTEN deficiency was significantly associated with genetic alterations. PTEN homozygous deletions or frameshift mutations typically result in absent protein expression; thus, we advocate for IHC as the initial screening method. When sample availability allows, both IHC and NGS should be conducted to ensure comprehensive assessment.
Additionally, analysis of the Genomics of Drug Sensitivity in Cancer and the Cancer Therapeutics Response Portal databases revealed that PTEN loss enhances the sensitivity of proteasome inhibitors across various tumours, indicating that our findings may have broad applicability.7 Similar cellular and animal phenotypes have been observed in gallbladder cancer4 and glioblastoma,11 suggesting that precision therapeutic approaches based on PTEN molecular subtyping with proteasome inhibitors may be extended to other tumours, benefiting more patients with PTEN deficiency.
In summary, our research demonstrates that bortezomib shows promising efficacy with manageable toxicity as a second-line therapy for PTEN-deficient iCCA, with manageable toxicity and a median OS of 9.6 months in the PP cohort. These results support the broaden application of proteasome inhibitors in solid tumours and provide renewed hope for patients with PTEN-deficient malignancies.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
