Craig D Newgard, Amber Lin, Jeremy D Goldhaber-Fiebert, Katherine E Remick, Marianne Gausche-Hill, Randall S Burd, Susan Malveau, Jennifer N B Cook, Peter C Jenkins, Stefanie G Ames, N Clay Mann, Nina E Glass, Hilary A Hewes, Mary Fallat, Apoorva Salvi, Brendan G Carr, K John McConnell, Caroline Q Stephens, Rachel Ford, Marc A Auerbach, Sean Babcock, Nathan Kuppermann
{"title":"各州和全国对急诊科儿科准备工作成本和挽救生命的估计。","authors":"Craig D Newgard, Amber Lin, Jeremy D Goldhaber-Fiebert, Katherine E Remick, Marianne Gausche-Hill, Randall S Burd, Susan Malveau, Jennifer N B Cook, Peter C Jenkins, Stefanie G Ames, N Clay Mann, Nina E Glass, Hilary A Hewes, Mary Fallat, Apoorva Salvi, Brendan G Carr, K John McConnell, Caroline Q Stephens, Rachel Ford, Marc A Auerbach, Sean Babcock, Nathan Kuppermann","doi":"10.1001/jamanetworkopen.2024.42154","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>High emergency department (ED) pediatric readiness is associated with improved survival among children receiving emergency care, but state and national costs to reach high ED readiness and the resulting number of lives that may be saved are unknown.</p><p><strong>Objective: </strong>To estimate the state and national annual costs of raising all EDs to high pediatric readiness and the resulting number of pediatric lives that may be saved each year.</p><p><strong>Design, setting, and participants: </strong>This cohort study used data from EDs in 50 US states and the District of Columbia from 2012 through 2022. Eligible children were ages 0 to 17 years receiving emergency services in US EDs and requiring admission, transfer to another hospital for admission, or dying in the ED (collectively termed at-risk children). Data were analyzed from October 2023 to May 2024.</p><p><strong>Exposure: </strong>EDs considered to have high readiness, with a weighted pediatric readiness score of 88 or above (range 0 to 100, with higher numbers representing higher readiness).</p><p><strong>Main outcomes and measures: </strong>Annual hospital expenditures to reach high ED readiness from current levels and the resulting number of pediatric lives that may be saved through universal high ED readiness.</p><p><strong>Results: </strong>A total 842 of 4840 EDs (17.4%; range, 2.9% to 100% by state) had high pediatric readiness. The annual US cost for all EDs to reach high pediatric readiness from current levels was $207 335 302 (95% CI, $188 401 692-$226 268 912), ranging from $0 to $11.84 per child by state. Of the 7619 child deaths occurring annually after presentation, 2143 (28.1%; 95% CI, 678-3608) were preventable through universal high ED pediatric readiness, with population-adjusted state estimates ranging from 0 to 69 pediatric lives per year.</p><p><strong>Conclusions and relevance: </strong>In this cohort study, raising all EDs to high pediatric readiness was estimated to prevent more than one-quarter of deaths among children receiving emergency services, with modest financial investment. State and national policies that raise ED pediatric readiness may save thousands of children's lives each year.</p>","PeriodicalId":14694,"journal":{"name":"JAMA Network Open","volume":"7 11","pages":"e2442154"},"PeriodicalIF":11.7000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530936/pdf/","citationCount":"0","resultStr":"{\"title\":\"State and National Estimates of the Cost of Emergency Department Pediatric Readiness and Lives Saved.\",\"authors\":\"Craig D Newgard, Amber Lin, Jeremy D Goldhaber-Fiebert, Katherine E Remick, Marianne Gausche-Hill, Randall S Burd, Susan Malveau, Jennifer N B Cook, Peter C Jenkins, Stefanie G Ames, N Clay Mann, Nina E Glass, Hilary A Hewes, Mary Fallat, Apoorva Salvi, Brendan G Carr, K John McConnell, Caroline Q Stephens, Rachel Ford, Marc A Auerbach, Sean Babcock, Nathan Kuppermann\",\"doi\":\"10.1001/jamanetworkopen.2024.42154\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>High emergency department (ED) pediatric readiness is associated with improved survival among children receiving emergency care, but state and national costs to reach high ED readiness and the resulting number of lives that may be saved are unknown.</p><p><strong>Objective: </strong>To estimate the state and national annual costs of raising all EDs to high pediatric readiness and the resulting number of pediatric lives that may be saved each year.</p><p><strong>Design, setting, and participants: </strong>This cohort study used data from EDs in 50 US states and the District of Columbia from 2012 through 2022. Eligible children were ages 0 to 17 years receiving emergency services in US EDs and requiring admission, transfer to another hospital for admission, or dying in the ED (collectively termed at-risk children). Data were analyzed from October 2023 to May 2024.</p><p><strong>Exposure: </strong>EDs considered to have high readiness, with a weighted pediatric readiness score of 88 or above (range 0 to 100, with higher numbers representing higher readiness).</p><p><strong>Main outcomes and measures: </strong>Annual hospital expenditures to reach high ED readiness from current levels and the resulting number of pediatric lives that may be saved through universal high ED readiness.</p><p><strong>Results: </strong>A total 842 of 4840 EDs (17.4%; range, 2.9% to 100% by state) had high pediatric readiness. The annual US cost for all EDs to reach high pediatric readiness from current levels was $207 335 302 (95% CI, $188 401 692-$226 268 912), ranging from $0 to $11.84 per child by state. Of the 7619 child deaths occurring annually after presentation, 2143 (28.1%; 95% CI, 678-3608) were preventable through universal high ED pediatric readiness, with population-adjusted state estimates ranging from 0 to 69 pediatric lives per year.</p><p><strong>Conclusions and relevance: </strong>In this cohort study, raising all EDs to high pediatric readiness was estimated to prevent more than one-quarter of deaths among children receiving emergency services, with modest financial investment. State and national policies that raise ED pediatric readiness may save thousands of children's lives each year.</p>\",\"PeriodicalId\":14694,\"journal\":{\"name\":\"JAMA Network Open\",\"volume\":\"7 11\",\"pages\":\"e2442154\"},\"PeriodicalIF\":11.7000,\"publicationDate\":\"2024-11-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530936/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Network Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamanetworkopen.2024.42154\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Network Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamanetworkopen.2024.42154","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
State and National Estimates of the Cost of Emergency Department Pediatric Readiness and Lives Saved.
Importance: High emergency department (ED) pediatric readiness is associated with improved survival among children receiving emergency care, but state and national costs to reach high ED readiness and the resulting number of lives that may be saved are unknown.
Objective: To estimate the state and national annual costs of raising all EDs to high pediatric readiness and the resulting number of pediatric lives that may be saved each year.
Design, setting, and participants: This cohort study used data from EDs in 50 US states and the District of Columbia from 2012 through 2022. Eligible children were ages 0 to 17 years receiving emergency services in US EDs and requiring admission, transfer to another hospital for admission, or dying in the ED (collectively termed at-risk children). Data were analyzed from October 2023 to May 2024.
Exposure: EDs considered to have high readiness, with a weighted pediatric readiness score of 88 or above (range 0 to 100, with higher numbers representing higher readiness).
Main outcomes and measures: Annual hospital expenditures to reach high ED readiness from current levels and the resulting number of pediatric lives that may be saved through universal high ED readiness.
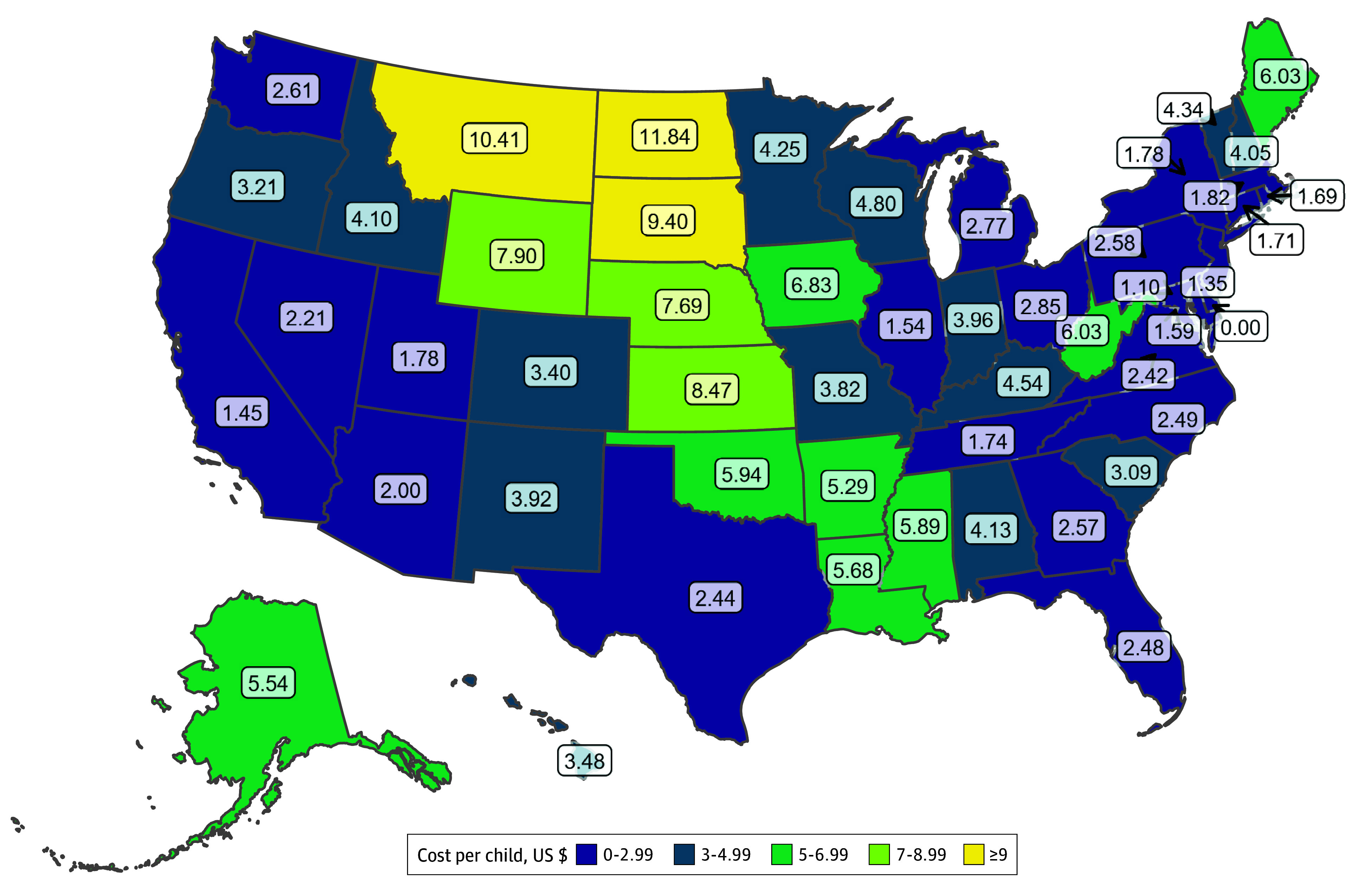
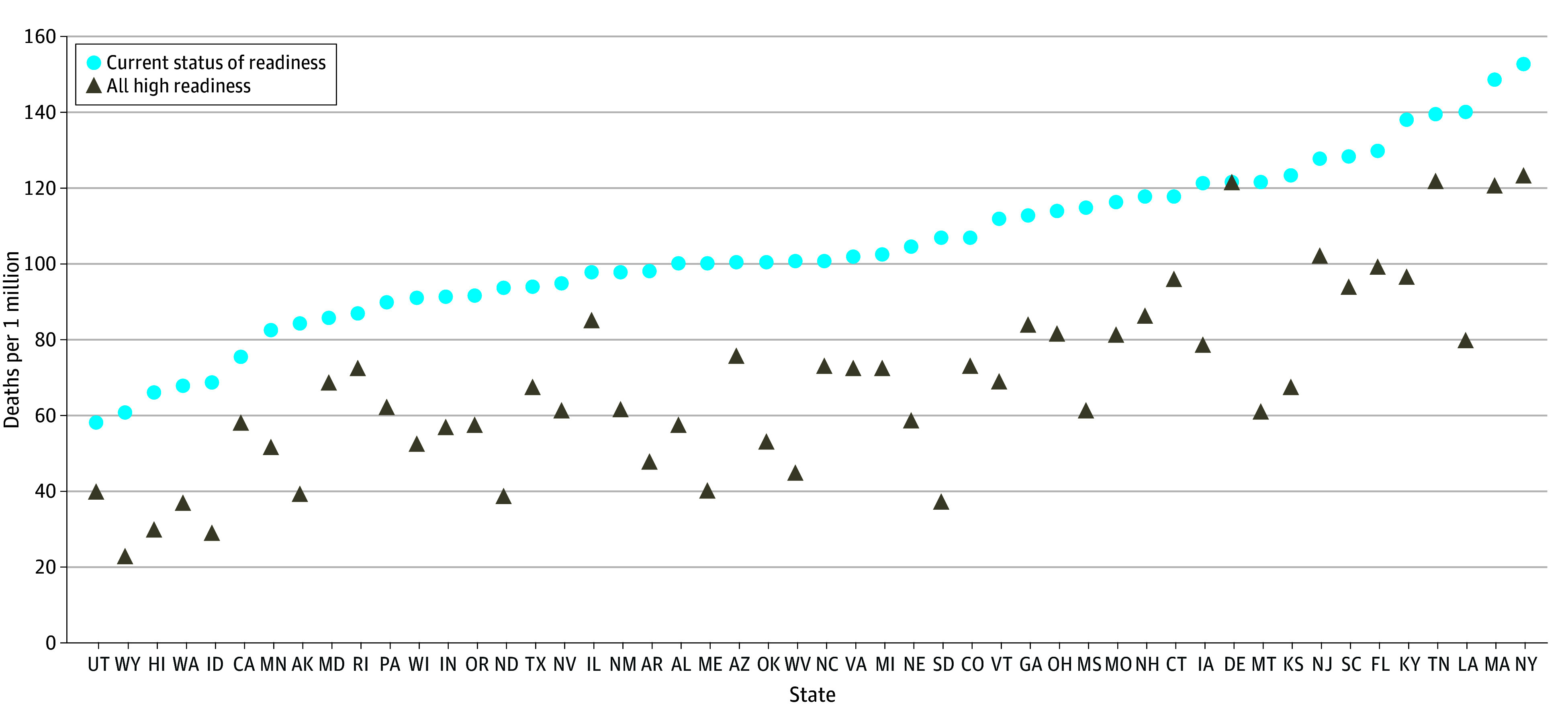
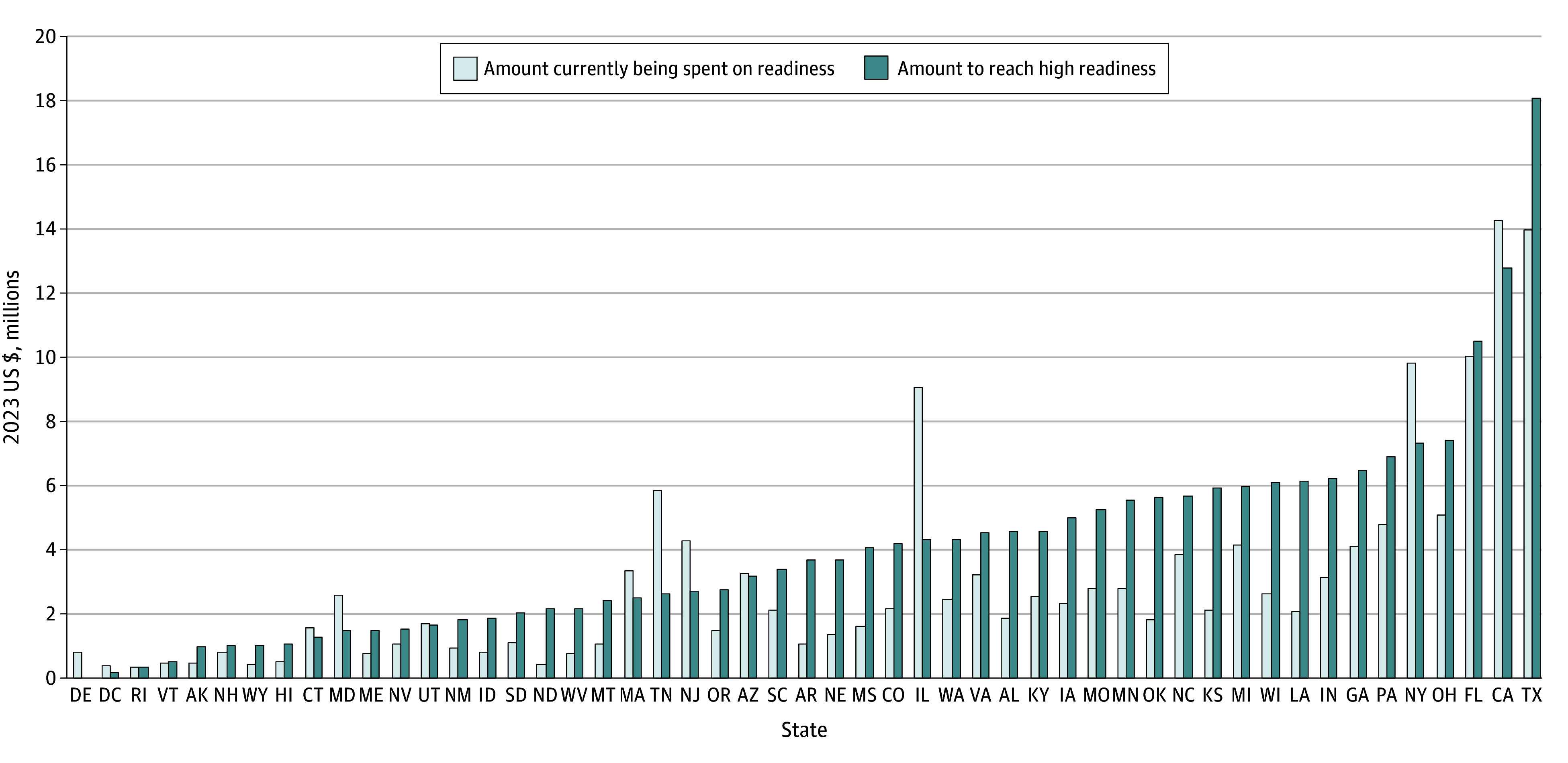
Results: A total 842 of 4840 EDs (17.4%; range, 2.9% to 100% by state) had high pediatric readiness. The annual US cost for all EDs to reach high pediatric readiness from current levels was $207 335 302 (95% CI, $188 401 692-$226 268 912), ranging from $0 to $11.84 per child by state. Of the 7619 child deaths occurring annually after presentation, 2143 (28.1%; 95% CI, 678-3608) were preventable through universal high ED pediatric readiness, with population-adjusted state estimates ranging from 0 to 69 pediatric lives per year.
Conclusions and relevance: In this cohort study, raising all EDs to high pediatric readiness was estimated to prevent more than one-quarter of deaths among children receiving emergency services, with modest financial investment. State and national policies that raise ED pediatric readiness may save thousands of children's lives each year.
期刊介绍:
JAMA Network Open, a member of the esteemed JAMA Network, stands as an international, peer-reviewed, open-access general medical journal.The publication is dedicated to disseminating research across various health disciplines and countries, encompassing clinical care, innovation in health care, health policy, and global health.
JAMA Network Open caters to clinicians, investigators, and policymakers, providing a platform for valuable insights and advancements in the medical field. As part of the JAMA Network, a consortium of peer-reviewed general medical and specialty publications, JAMA Network Open contributes to the collective knowledge and understanding within the medical community.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
