Mohsin Fayaz, Sarabjit Singh Chibber, Kaushal Deep Singh, Lamkordor Tyngkam, Amir Hela, Bipin Chaurasia
{"title":"利用徒手技术和术中 C 型臂成像技术的细微差别,实现 650 枚经关节螺钉的空前之旅。","authors":"Mohsin Fayaz, Sarabjit Singh Chibber, Kaushal Deep Singh, Lamkordor Tyngkam, Amir Hela, Bipin Chaurasia","doi":"10.4103/jcvjs.jcvjs_56_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pedicle screw placement plays a crucial role in treating various cases such as fractures, scoliosis, degenerative spine issues, and kyphosis, reinforcing all three spinal columns simultaneously. While three-dimensional navigation-assisted pedicle screw placement is considered superior, the freehand technique relies on anatomical landmarks and tactile feedback, with observed low complication rates.</p><p><strong>Materials and methods: </strong>This was a prospective single-center study conducted over a period of 3 years. It included all patients of dorsal, lumbar, and sacral spinal instability of myriad etiology. Previously operated patients and sick obtunded patients were excluded from the study.</p><p><strong>Results: </strong>In our study, we included 102 patients including 62 (60.7%) males and 40 (39.2%) females. More than half of patients were young in the age group of 20-50 years. Our study population had a varied etiology with 43.1% of patients having vertebral column instability due to trauma. The other etiologies were spondylolisthesis and lumbar canal stenosis (39.2%), Pott's spine (11.7%), tumors (2.9%), and osteoporotic fractures (2.9%). Majority of patients (44.1%) presented with lower backache with radiculopathy. All the transpedicular screws inserted were evaluated by C-arm to assess for screw fixation. In the first year of our study, an average of 4 anteroposterior (AP) and 4 lateral C-arm X-ray shots were taken per screw placement. In the next year, an average of 3 AP and 3 lateral shots and finally in the last year of our study only 2 AP and 2 lateral C-arm X-ray shots were taken per screw placement. Out of 650 screws placed, 4 screws were identified to cause breach with maximum breaches in the lumbar spine fixation. In dorsal spine fixation, there was 1 lateral breach at D10. In lumbar spine fixation, there were 3 breaches: two medial one each at L4 and L5 and one anterior at L2 level. The various complications include wound infection, temporary and permanent neurological deficit, screw breakage, screw misplacement, cerebrospinal fluid leaks, nonunion, and spinal epidural hematoma.</p><p><strong>Conclusions: </strong>Our study has provided strong encouragement to persist with the freehand technique in transpedicular fixation surgeries after a certain number of cases given the minimal breaches and complications observed. There are subtle technical nuances as we increase the number of cases with less exposure of anatomical landmarks and X-rays. Success hinges on experience, adherence to technique, and thorough preoperative planning. Further research and extended follow-up periods are necessary to firmly establish this technique as the gold standard.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"15 3","pages":"326-330"},"PeriodicalIF":1.3000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11524549/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unprecedented journey to 650 transpedicular screws using freehand technique and intraoperative C-arm imaging with technical nuances.\",\"authors\":\"Mohsin Fayaz, Sarabjit Singh Chibber, Kaushal Deep Singh, Lamkordor Tyngkam, Amir Hela, Bipin Chaurasia\",\"doi\":\"10.4103/jcvjs.jcvjs_56_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Pedicle screw placement plays a crucial role in treating various cases such as fractures, scoliosis, degenerative spine issues, and kyphosis, reinforcing all three spinal columns simultaneously. While three-dimensional navigation-assisted pedicle screw placement is considered superior, the freehand technique relies on anatomical landmarks and tactile feedback, with observed low complication rates.</p><p><strong>Materials and methods: </strong>This was a prospective single-center study conducted over a period of 3 years. It included all patients of dorsal, lumbar, and sacral spinal instability of myriad etiology. Previously operated patients and sick obtunded patients were excluded from the study.</p><p><strong>Results: </strong>In our study, we included 102 patients including 62 (60.7%) males and 40 (39.2%) females. More than half of patients were young in the age group of 20-50 years. Our study population had a varied etiology with 43.1% of patients having vertebral column instability due to trauma. The other etiologies were spondylolisthesis and lumbar canal stenosis (39.2%), Pott's spine (11.7%), tumors (2.9%), and osteoporotic fractures (2.9%). Majority of patients (44.1%) presented with lower backache with radiculopathy. All the transpedicular screws inserted were evaluated by C-arm to assess for screw fixation. In the first year of our study, an average of 4 anteroposterior (AP) and 4 lateral C-arm X-ray shots were taken per screw placement. In the next year, an average of 3 AP and 3 lateral shots and finally in the last year of our study only 2 AP and 2 lateral C-arm X-ray shots were taken per screw placement. Out of 650 screws placed, 4 screws were identified to cause breach with maximum breaches in the lumbar spine fixation. In dorsal spine fixation, there was 1 lateral breach at D10. In lumbar spine fixation, there were 3 breaches: two medial one each at L4 and L5 and one anterior at L2 level. The various complications include wound infection, temporary and permanent neurological deficit, screw breakage, screw misplacement, cerebrospinal fluid leaks, nonunion, and spinal epidural hematoma.</p><p><strong>Conclusions: </strong>Our study has provided strong encouragement to persist with the freehand technique in transpedicular fixation surgeries after a certain number of cases given the minimal breaches and complications observed. There are subtle technical nuances as we increase the number of cases with less exposure of anatomical landmarks and X-rays. Success hinges on experience, adherence to technique, and thorough preoperative planning. Further research and extended follow-up periods are necessary to firmly establish this technique as the gold standard.</p>\",\"PeriodicalId\":51721,\"journal\":{\"name\":\"Journal of Craniovertebral Junction and Spine\",\"volume\":\"15 3\",\"pages\":\"326-330\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11524549/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Craniovertebral Junction and Spine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcvjs.jcvjs_56_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_56_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
简介椎弓根螺钉置入术在治疗骨折、脊柱侧弯、脊柱退行性问题和驼背等各种病例中发挥着至关重要的作用,可同时加固三根脊柱。虽然三维导航辅助椎弓根螺钉置入术被认为更优越,但徒手技术依赖于解剖标志和触觉反馈,并发症发生率较低:这是一项为期三年的前瞻性单中心研究。材料:这是一项为期 3 年的前瞻性单中心研究,研究对象包括各种病因引起的背椎、腰椎和骶椎不稳的所有患者。研究排除了曾接受过手术的患者和患病昏迷的患者:研究共纳入 102 名患者,其中男性 62 名(60.7%),女性 40 名(39.2%)。一半以上的患者年龄在 20-50 岁之间。我们的研究对象病因多样,43.1%的患者因外伤导致椎体不稳。其他病因包括脊柱滑脱症和腰椎管狭窄(39.2%)、Pott's 脊柱(11.7%)、肿瘤(2.9%)和骨质疏松性骨折(2.9%)。大多数患者(44.1%)的症状是下背部疼痛并伴有根性病变。所有插入的经关节螺钉均通过C型臂进行评估,以确定螺钉是否固定。在研究的第一年,每次植入螺钉平均需要拍摄 4 张正侧位(AP)和 4 张侧位 C 型臂 X 光片。第二年,平均拍摄了 3 张正侧位和 3 张侧位 X 光片,而在研究的最后一年,每次放置螺钉只拍摄了 2 张正侧位和 2 张侧位 C 型臂 X 光片。在安放的 650 颗螺钉中,有 4 颗螺钉被确认会造成破损,其中腰椎固定的破损最多。在背椎固定中,D10 处有 1 处侧向破损。在腰椎固定中,有 3 处破损:两处内侧,分别位于 L4 和 L5,一处前侧,位于 L2 水平。各种并发症包括伤口感染、暂时性和永久性神经功能缺损、螺钉断裂、螺钉错位、脑脊液漏、不愈合和脊髓硬膜外血肿:鉴于观察到的破损和并发症极少,我们的研究有力地鼓励了在经椎弓根固定手术中坚持使用徒手技术。随着病例数量的增加,解剖标志和 X 光片的暴露程度降低,技术上会出现一些细微的差别。成功与否取决于经验、对技术的坚持和周密的术前计划。要将这种技术牢固地确立为黄金标准,还需要进一步的研究和更长时间的随访。
Unprecedented journey to 650 transpedicular screws using freehand technique and intraoperative C-arm imaging with technical nuances.
Introduction: Pedicle screw placement plays a crucial role in treating various cases such as fractures, scoliosis, degenerative spine issues, and kyphosis, reinforcing all three spinal columns simultaneously. While three-dimensional navigation-assisted pedicle screw placement is considered superior, the freehand technique relies on anatomical landmarks and tactile feedback, with observed low complication rates.
Materials and methods: This was a prospective single-center study conducted over a period of 3 years. It included all patients of dorsal, lumbar, and sacral spinal instability of myriad etiology. Previously operated patients and sick obtunded patients were excluded from the study.
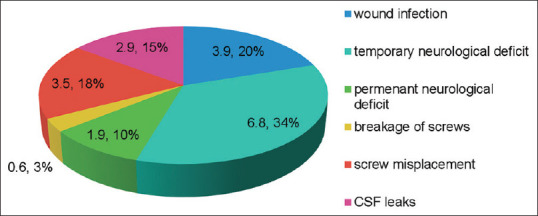
Results: In our study, we included 102 patients including 62 (60.7%) males and 40 (39.2%) females. More than half of patients were young in the age group of 20-50 years. Our study population had a varied etiology with 43.1% of patients having vertebral column instability due to trauma. The other etiologies were spondylolisthesis and lumbar canal stenosis (39.2%), Pott's spine (11.7%), tumors (2.9%), and osteoporotic fractures (2.9%). Majority of patients (44.1%) presented with lower backache with radiculopathy. All the transpedicular screws inserted were evaluated by C-arm to assess for screw fixation. In the first year of our study, an average of 4 anteroposterior (AP) and 4 lateral C-arm X-ray shots were taken per screw placement. In the next year, an average of 3 AP and 3 lateral shots and finally in the last year of our study only 2 AP and 2 lateral C-arm X-ray shots were taken per screw placement. Out of 650 screws placed, 4 screws were identified to cause breach with maximum breaches in the lumbar spine fixation. In dorsal spine fixation, there was 1 lateral breach at D10. In lumbar spine fixation, there were 3 breaches: two medial one each at L4 and L5 and one anterior at L2 level. The various complications include wound infection, temporary and permanent neurological deficit, screw breakage, screw misplacement, cerebrospinal fluid leaks, nonunion, and spinal epidural hematoma.
Conclusions: Our study has provided strong encouragement to persist with the freehand technique in transpedicular fixation surgeries after a certain number of cases given the minimal breaches and complications observed. There are subtle technical nuances as we increase the number of cases with less exposure of anatomical landmarks and X-rays. Success hinges on experience, adherence to technique, and thorough preoperative planning. Further research and extended follow-up periods are necessary to firmly establish this technique as the gold standard.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
