Cynthia A King, Benjamin S King, Tara Nagaraj, M Dave Gothard
{"title":"药剂师指导基层诊所糖尿病管理的成本效益分析。","authors":"Cynthia A King, Benjamin S King, Tara Nagaraj, M Dave Gothard","doi":"10.24926/iip.v15i3.6300","DOIUrl":null,"url":null,"abstract":"<p><p><i>Purpose:</i> Ambulatory care pharmacists (ACPs) on healthcare teams improve patient outcomes and can manage multiple chronic disease states. ACPs have demonstrated clinical benefit but need to prove financial sustainability. The primary objective of this study was to determine the cost-effectiveness of utilizing ACPs for diabetes mellitus (DM) management. <i>Methods:</i> This was a quasi-experimental, retrospective, single health system, multi-clinic cohort study of 406 patients living with DM, ≥ 18 years of age, with a HbA1c of ≥ 8%, receiving primary care services within an academic health system between May 2015 to March 2018. In the ACP group, the ACP was part of the care team for DM management while in the PCP group, patients were managed only by a PCP with or without an endocrinologist (usual care). The incremental cost-effectiveness ratio (ICER) was calculated to determine the clinic-associated cost of an ACP-led DM management clinic. <i>Results:</i> Based on the ICER calculation, clinic-associated cost for ACP-led DM management was $126 per patient per year for each additional HbA1c percent lowered. Additional ICER calculations demonstrated the clinic-associated cost to move one patient with HbA1c ≥9% to HbA1c < 9% was $612. Change in HbA1c over 12 months was -2.5% in the ACP group and in the PCP group +1.08% (p<0.001). Based on quality metrics at 12-months, the ACP group met the goal of 75% of patients having a HbA1c < 9% and being prescribed a statin vs. the PCP group only met the metric for statin use. Based on facility fee billing, the ACPs cover approximately 70% of their annual salary and benefits from face-to-face visits. <i>Conclusions:</i> ACPs led to significantly improved clinical outcomes with marginal up-front costs that could lead potential future cost savings through reductions in DM related complications or improving incentivized returns by achieving goal quality metric levels.</p>","PeriodicalId":501014,"journal":{"name":"Innovations in pharmacy","volume":"15 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11524212/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness Analysis of Pharmacist-Led Diabetes Management Across Primary Care Clinics.\",\"authors\":\"Cynthia A King, Benjamin S King, Tara Nagaraj, M Dave Gothard\",\"doi\":\"10.24926/iip.v15i3.6300\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><i>Purpose:</i> Ambulatory care pharmacists (ACPs) on healthcare teams improve patient outcomes and can manage multiple chronic disease states. ACPs have demonstrated clinical benefit but need to prove financial sustainability. The primary objective of this study was to determine the cost-effectiveness of utilizing ACPs for diabetes mellitus (DM) management. <i>Methods:</i> This was a quasi-experimental, retrospective, single health system, multi-clinic cohort study of 406 patients living with DM, ≥ 18 years of age, with a HbA1c of ≥ 8%, receiving primary care services within an academic health system between May 2015 to March 2018. In the ACP group, the ACP was part of the care team for DM management while in the PCP group, patients were managed only by a PCP with or without an endocrinologist (usual care). The incremental cost-effectiveness ratio (ICER) was calculated to determine the clinic-associated cost of an ACP-led DM management clinic. <i>Results:</i> Based on the ICER calculation, clinic-associated cost for ACP-led DM management was $126 per patient per year for each additional HbA1c percent lowered. Additional ICER calculations demonstrated the clinic-associated cost to move one patient with HbA1c ≥9% to HbA1c < 9% was $612. Change in HbA1c over 12 months was -2.5% in the ACP group and in the PCP group +1.08% (p<0.001). Based on quality metrics at 12-months, the ACP group met the goal of 75% of patients having a HbA1c < 9% and being prescribed a statin vs. the PCP group only met the metric for statin use. Based on facility fee billing, the ACPs cover approximately 70% of their annual salary and benefits from face-to-face visits. <i>Conclusions:</i> ACPs led to significantly improved clinical outcomes with marginal up-front costs that could lead potential future cost savings through reductions in DM related complications or improving incentivized returns by achieving goal quality metric levels.</p>\",\"PeriodicalId\":501014,\"journal\":{\"name\":\"Innovations in pharmacy\",\"volume\":\"15 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11524212/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Innovations in pharmacy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24926/iip.v15i3.6300\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovations in pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24926/iip.v15i3.6300","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Cost-Effectiveness Analysis of Pharmacist-Led Diabetes Management Across Primary Care Clinics.
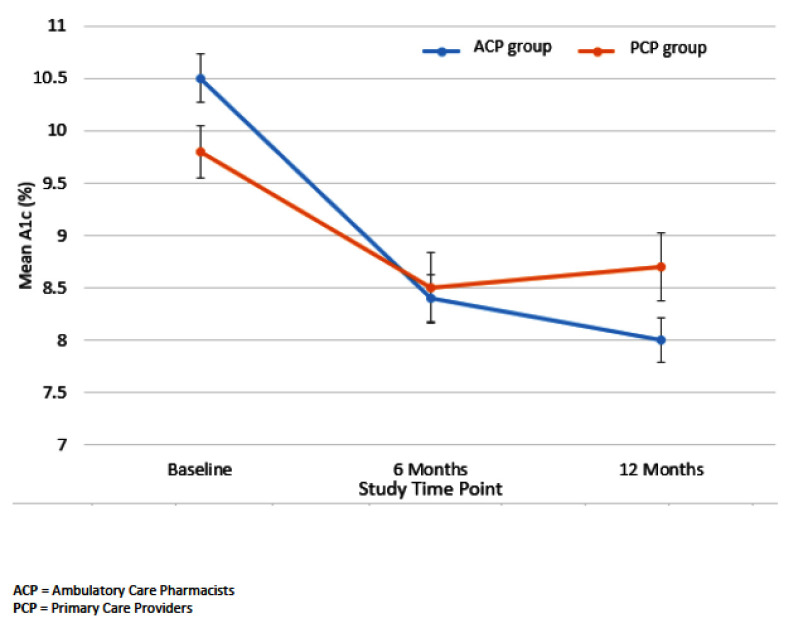
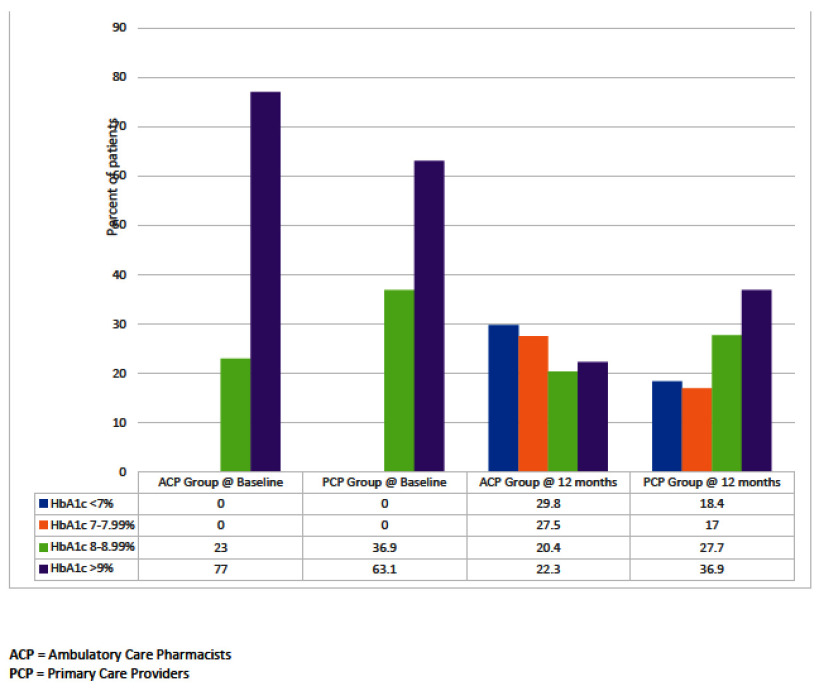
Purpose: Ambulatory care pharmacists (ACPs) on healthcare teams improve patient outcomes and can manage multiple chronic disease states. ACPs have demonstrated clinical benefit but need to prove financial sustainability. The primary objective of this study was to determine the cost-effectiveness of utilizing ACPs for diabetes mellitus (DM) management. Methods: This was a quasi-experimental, retrospective, single health system, multi-clinic cohort study of 406 patients living with DM, ≥ 18 years of age, with a HbA1c of ≥ 8%, receiving primary care services within an academic health system between May 2015 to March 2018. In the ACP group, the ACP was part of the care team for DM management while in the PCP group, patients were managed only by a PCP with or without an endocrinologist (usual care). The incremental cost-effectiveness ratio (ICER) was calculated to determine the clinic-associated cost of an ACP-led DM management clinic. Results: Based on the ICER calculation, clinic-associated cost for ACP-led DM management was $126 per patient per year for each additional HbA1c percent lowered. Additional ICER calculations demonstrated the clinic-associated cost to move one patient with HbA1c ≥9% to HbA1c < 9% was $612. Change in HbA1c over 12 months was -2.5% in the ACP group and in the PCP group +1.08% (p<0.001). Based on quality metrics at 12-months, the ACP group met the goal of 75% of patients having a HbA1c < 9% and being prescribed a statin vs. the PCP group only met the metric for statin use. Based on facility fee billing, the ACPs cover approximately 70% of their annual salary and benefits from face-to-face visits. Conclusions: ACPs led to significantly improved clinical outcomes with marginal up-front costs that could lead potential future cost savings through reductions in DM related complications or improving incentivized returns by achieving goal quality metric levels.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
