Doris K. Hansen, Santosh Gautam, Marie-Hélène Lafeuille, Carmine Rossi, Bronwyn Moore, Anabelle Tardif-Samson, Philippe Thompson-Leduc, Alex Z. Fu, Annelore Cortoos, Shuchita Kaila, Rafael Fonseca
{"title":"符合移植条件的多发性骨髓瘤患者接受前线达拉曲单抗、来那度胺和地塞米松(DRd)与硼替佐米、来那度胺和地塞米松(VRd)治疗后到下一次治疗或死亡的时间比较。","authors":"Doris K. Hansen, Santosh Gautam, Marie-Hélène Lafeuille, Carmine Rossi, Bronwyn Moore, Anabelle Tardif-Samson, Philippe Thompson-Leduc, Alex Z. Fu, Annelore Cortoos, Shuchita Kaila, Rafael Fonseca","doi":"10.1002/cam4.70308","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Daratumumab, lenalidomide, and dexamethasone (DRd) and bortezomib, lenalidomide, and dexamethasone (VRd) are the only preferred treatment regimens for patients with transplant-ineligible (TIE) newly diagnosed multiple myeloma (NDMM). As there are no randomized head-to-head studies of DRd versus VRd, this analysis aimed to compare real-world time-to-next-treatment (TTNT) or death in this population.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients with NDMM who received front-line (FL) DRd or VRd were identified from the Acentrus database (January 1, 2018 to May 31, 2023). Those with a record of a stem cell transplant or aged < 65 years were excluded to limit analysis to the TIE population. Inverse probability of treatment weighting was used to balance baseline patient characteristics. A doubly robust Cox proportional hazards model was used to compare TTNT or death between cohorts.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 149 and 494 patients who initiated DRd and VRd, respectively, were identified. After weighting (weighted N<sub>DRd</sub> = 302, weighted N<sub>VRd</sub> = 341), cohorts had similar baseline characteristics. Of these, 98 (32.4%) DRd and 175 (51.2%) VRd patients either received a subsequent line of therapy or died, with a median TTNT or death of 37.8 months in the DRd cohort and 18.7 months in the VRd cohort (hazard ratio: 0.58, 95% confidence interval: 0.35, 0.81; <i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Treatment of TIE NDMM patients with DRd led to a significantly longer TTNT or death compared to VRd, evidenced by a 42% risk reduction, supporting the effectiveness of DRd over VRd as FL treatment in this patient population.</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"13 21","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530241/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Time to Next Treatment or Death Between Front-Line Daratumumab, Lenalidomide, and Dexamethasone (DRd) Versus Bortezomib, Lenalidomide, and Dexamethasone (VRd) Among Transplant-Ineligible Patients With Multiple Myeloma\",\"authors\":\"Doris K. Hansen, Santosh Gautam, Marie-Hélène Lafeuille, Carmine Rossi, Bronwyn Moore, Anabelle Tardif-Samson, Philippe Thompson-Leduc, Alex Z. Fu, Annelore Cortoos, Shuchita Kaila, Rafael Fonseca\",\"doi\":\"10.1002/cam4.70308\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Introduction</h3>\\n \\n <p>Daratumumab, lenalidomide, and dexamethasone (DRd) and bortezomib, lenalidomide, and dexamethasone (VRd) are the only preferred treatment regimens for patients with transplant-ineligible (TIE) newly diagnosed multiple myeloma (NDMM). As there are no randomized head-to-head studies of DRd versus VRd, this analysis aimed to compare real-world time-to-next-treatment (TTNT) or death in this population.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Patients with NDMM who received front-line (FL) DRd or VRd were identified from the Acentrus database (January 1, 2018 to May 31, 2023). Those with a record of a stem cell transplant or aged < 65 years were excluded to limit analysis to the TIE population. Inverse probability of treatment weighting was used to balance baseline patient characteristics. A doubly robust Cox proportional hazards model was used to compare TTNT or death between cohorts.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 149 and 494 patients who initiated DRd and VRd, respectively, were identified. After weighting (weighted N<sub>DRd</sub> = 302, weighted N<sub>VRd</sub> = 341), cohorts had similar baseline characteristics. Of these, 98 (32.4%) DRd and 175 (51.2%) VRd patients either received a subsequent line of therapy or died, with a median TTNT or death of 37.8 months in the DRd cohort and 18.7 months in the VRd cohort (hazard ratio: 0.58, 95% confidence interval: 0.35, 0.81; <i>p</i> < 0.001).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Treatment of TIE NDMM patients with DRd led to a significantly longer TTNT or death compared to VRd, evidenced by a 42% risk reduction, supporting the effectiveness of DRd over VRd as FL treatment in this patient population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":139,\"journal\":{\"name\":\"Cancer Medicine\",\"volume\":\"13 21\",\"pages\":\"\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530241/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70308\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70308","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Comparison of Time to Next Treatment or Death Between Front-Line Daratumumab, Lenalidomide, and Dexamethasone (DRd) Versus Bortezomib, Lenalidomide, and Dexamethasone (VRd) Among Transplant-Ineligible Patients With Multiple Myeloma
Introduction
Daratumumab, lenalidomide, and dexamethasone (DRd) and bortezomib, lenalidomide, and dexamethasone (VRd) are the only preferred treatment regimens for patients with transplant-ineligible (TIE) newly diagnosed multiple myeloma (NDMM). As there are no randomized head-to-head studies of DRd versus VRd, this analysis aimed to compare real-world time-to-next-treatment (TTNT) or death in this population.
Methods
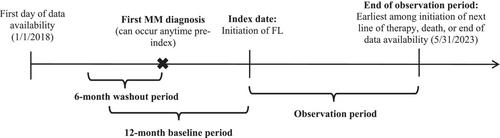
Patients with NDMM who received front-line (FL) DRd or VRd were identified from the Acentrus database (January 1, 2018 to May 31, 2023). Those with a record of a stem cell transplant or aged < 65 years were excluded to limit analysis to the TIE population. Inverse probability of treatment weighting was used to balance baseline patient characteristics. A doubly robust Cox proportional hazards model was used to compare TTNT or death between cohorts.
Results
A total of 149 and 494 patients who initiated DRd and VRd, respectively, were identified. After weighting (weighted NDRd = 302, weighted NVRd = 341), cohorts had similar baseline characteristics. Of these, 98 (32.4%) DRd and 175 (51.2%) VRd patients either received a subsequent line of therapy or died, with a median TTNT or death of 37.8 months in the DRd cohort and 18.7 months in the VRd cohort (hazard ratio: 0.58, 95% confidence interval: 0.35, 0.81; p < 0.001).
Conclusion
Treatment of TIE NDMM patients with DRd led to a significantly longer TTNT or death compared to VRd, evidenced by a 42% risk reduction, supporting the effectiveness of DRd over VRd as FL treatment in this patient population.
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
