Rahul C Deo, Rebecca Smith, Calum A MacRae, Esha Price, Horace Sheffield, Rahul Patel
{"title":"软件驱动的慢性病管理:社区血压控制试点中的算法设计与实施。","authors":"Rahul C Deo, Rebecca Smith, Calum A MacRae, Esha Price, Horace Sheffield, Rahul Patel","doi":"10.1177/20503121241284025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Optimal guideline-directed medical therapy is rarely attained in practice, resulting in inadequate control of diseases such as hypertension, with poorer results in under-resourced communities. Technology, including artificial intelligence-driven decision support and software-driven workflow transformation, can potentially improve disease outcomes at a reduced cost, although it must be integrated with a holistic approach.</p><p><strong>Methods: </strong>We describe the design of a software platform that enables rapid iterative remote management of >20 conditions across cardiac-kidney-metabolic disease. The platform distributes work across a care team of providers and care navigators, automates decision-making, ordering, and documentation, supports rapid incorporation of new evidence, and launches pragmatic trials. We describe software used in a 500-person community-based blood pressure control implemented as a single-arm quality improvement program. The primary endpoint was the proportion of patients meeting the Healthcare Effectiveness Data and Information Set quality measure blood pressure goal (<140/90) at 12 weeks.</p><p><strong>Results: </strong>A total of 1609 patients were screened, 945 (59%) were found to have uncontrolled hypertension, and 512 patients consented to join the program. The average age was 61 ± 11 years; 59% were female, and 99% self-identified as Black. Blood pressure distribution was: 10% Stage 1 (SBP 130-139 mmHg or DBP 80-89 mmHg), 69% Stage 2 (SBP 140-179 mmHg or DBP 90-119 mmHg), and 21% Stage 3 (SBP >180 mmHg or DBP >120 mmHg). Two hundred four patients (39%) proceeded to a provider encounter, and 160 of these (78%) completed the program. The Healthcare Effectiveness Data and Information Set blood pressure goal was achieved in <12 weeks of enrollment for 141 participants (69% of those enrolled, 88% of those who completed the program).</p><p><strong>Conclusion: </strong>Software-driven remote blood pressure is feasible, although strategies to improve patient enrollment will be needed to achieve maximum impact. Future work will be required to compare outcomes to usual care and evaluate concurrent management of multiple cardiac-kidney-metabolic conditions.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"12 ","pages":"20503121241284025"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530998/pdf/","citationCount":"0","resultStr":"{\"title\":\"Software-driven chronic disease management: Algorithm design and implementation in a community-based blood pressure control pilot.\",\"authors\":\"Rahul C Deo, Rebecca Smith, Calum A MacRae, Esha Price, Horace Sheffield, Rahul Patel\",\"doi\":\"10.1177/20503121241284025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Optimal guideline-directed medical therapy is rarely attained in practice, resulting in inadequate control of diseases such as hypertension, with poorer results in under-resourced communities. Technology, including artificial intelligence-driven decision support and software-driven workflow transformation, can potentially improve disease outcomes at a reduced cost, although it must be integrated with a holistic approach.</p><p><strong>Methods: </strong>We describe the design of a software platform that enables rapid iterative remote management of >20 conditions across cardiac-kidney-metabolic disease. The platform distributes work across a care team of providers and care navigators, automates decision-making, ordering, and documentation, supports rapid incorporation of new evidence, and launches pragmatic trials. We describe software used in a 500-person community-based blood pressure control implemented as a single-arm quality improvement program. The primary endpoint was the proportion of patients meeting the Healthcare Effectiveness Data and Information Set quality measure blood pressure goal (<140/90) at 12 weeks.</p><p><strong>Results: </strong>A total of 1609 patients were screened, 945 (59%) were found to have uncontrolled hypertension, and 512 patients consented to join the program. The average age was 61 ± 11 years; 59% were female, and 99% self-identified as Black. Blood pressure distribution was: 10% Stage 1 (SBP 130-139 mmHg or DBP 80-89 mmHg), 69% Stage 2 (SBP 140-179 mmHg or DBP 90-119 mmHg), and 21% Stage 3 (SBP >180 mmHg or DBP >120 mmHg). Two hundred four patients (39%) proceeded to a provider encounter, and 160 of these (78%) completed the program. The Healthcare Effectiveness Data and Information Set blood pressure goal was achieved in <12 weeks of enrollment for 141 participants (69% of those enrolled, 88% of those who completed the program).</p><p><strong>Conclusion: </strong>Software-driven remote blood pressure is feasible, although strategies to improve patient enrollment will be needed to achieve maximum impact. Future work will be required to compare outcomes to usual care and evaluate concurrent management of multiple cardiac-kidney-metabolic conditions.</p>\",\"PeriodicalId\":21398,\"journal\":{\"name\":\"SAGE Open Medicine\",\"volume\":\"12 \",\"pages\":\"20503121241284025\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-10-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11530998/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAGE Open Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20503121241284025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121241284025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Software-driven chronic disease management: Algorithm design and implementation in a community-based blood pressure control pilot.
Background: Optimal guideline-directed medical therapy is rarely attained in practice, resulting in inadequate control of diseases such as hypertension, with poorer results in under-resourced communities. Technology, including artificial intelligence-driven decision support and software-driven workflow transformation, can potentially improve disease outcomes at a reduced cost, although it must be integrated with a holistic approach.
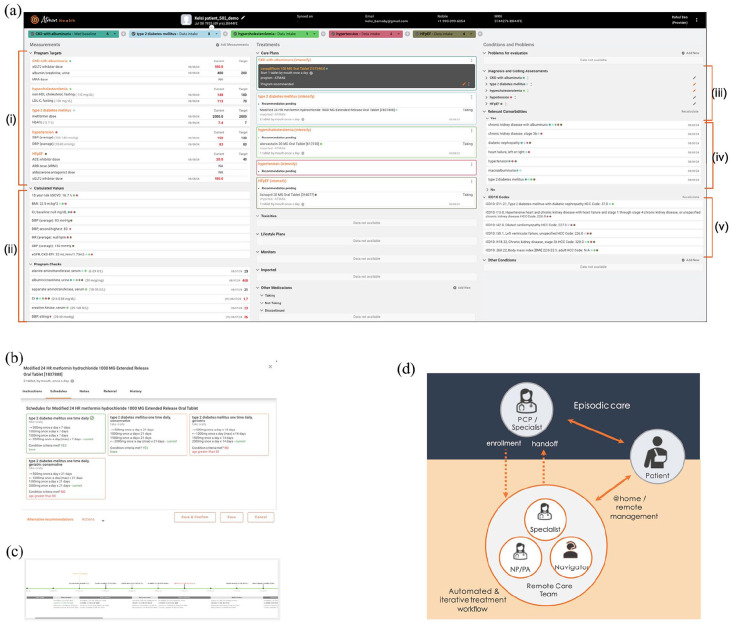
Methods: We describe the design of a software platform that enables rapid iterative remote management of >20 conditions across cardiac-kidney-metabolic disease. The platform distributes work across a care team of providers and care navigators, automates decision-making, ordering, and documentation, supports rapid incorporation of new evidence, and launches pragmatic trials. We describe software used in a 500-person community-based blood pressure control implemented as a single-arm quality improvement program. The primary endpoint was the proportion of patients meeting the Healthcare Effectiveness Data and Information Set quality measure blood pressure goal (<140/90) at 12 weeks.
Results: A total of 1609 patients were screened, 945 (59%) were found to have uncontrolled hypertension, and 512 patients consented to join the program. The average age was 61 ± 11 years; 59% were female, and 99% self-identified as Black. Blood pressure distribution was: 10% Stage 1 (SBP 130-139 mmHg or DBP 80-89 mmHg), 69% Stage 2 (SBP 140-179 mmHg or DBP 90-119 mmHg), and 21% Stage 3 (SBP >180 mmHg or DBP >120 mmHg). Two hundred four patients (39%) proceeded to a provider encounter, and 160 of these (78%) completed the program. The Healthcare Effectiveness Data and Information Set blood pressure goal was achieved in <12 weeks of enrollment for 141 participants (69% of those enrolled, 88% of those who completed the program).
Conclusion: Software-driven remote blood pressure is feasible, although strategies to improve patient enrollment will be needed to achieve maximum impact. Future work will be required to compare outcomes to usual care and evaluate concurrent management of multiple cardiac-kidney-metabolic conditions.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
