Luiz Carlos Almeida da Silva, Yusuke Hori, Burak Kaymaz, Kenneth J Rogers, Arianna Trionfo, James Richard Bowen, Jason J Howard, Michael Wade Shrader, Freeman Miller
{"title":"根据脑瘫和脊髓性肌肉萎缩症患儿神经功能受损的严重程度确定股骨颈轴角的变化。","authors":"Luiz Carlos Almeida da Silva, Yusuke Hori, Burak Kaymaz, Kenneth J Rogers, Arianna Trionfo, James Richard Bowen, Jason J Howard, Michael Wade Shrader, Freeman Miller","doi":"10.1177/18632521241277023","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The neck-shaft angle and head-shaft angle in children with varying levels of neurological disability were evaluated to define change over different ages.</p><p><strong>Methods: </strong>Children aged 1-12 years with spastic cerebral palsy, spinal muscular atrophy types 1 and 2, or typical development were reviewed to evaluate the neck-shaft angle and head-shaft angle. Patients were divided into five groups: Gross Motor Function Classification System levels I and II, Gross Motor Function Classification System level III, Gross Motor Function Classification System levels IV and V, spinal muscular atrophy types 1 and 2, and typical development. A linear mixed model was utilized to evaluate neck-shaft angle and head-shaft angle.</p><p><strong>Results: </strong>Data from 196 children (mean age 4.8 ± 4.5 years) were included. Gross Motor Function Classification System levels I and II: 22 children, 130 hip radiographs measured, neck-shaft angle 143.7 ± 7.4, and head-shaft angle 160.0 ± 7.1. Gross Motor Function Classification System level III: 8 children, 33 hips evaluated, neck-shaft angle 153.1 ± 4.3, and head-shaft angle 163.4 ± 4.2. Gross Motor Function Classification System levels IV and V: 30 children, 137 hip radiographs measured, neck-shaft angle 156.4 ± 5.6, and head-shaft angle 167.9 ± 6.8. Spinal muscular atrophy types 1 and 2: 32 children, 83 hip radiographs measured, neck-shaft angle 161.9 ± 9.7, and head-shaft angle 173.4 ± 7.4. Typical development: 104 children, 222 hip radiographs measured, neck-shaft angle 138.6 ± 7.0, and head-shaft angle 156.4 ± 5.9. There were significant statistical differences when comparing neck-shaft angle and head-shaft angle.</p><p><strong>Conclusion: </strong>As children grow, neck-shaft angle and head-shaft angle tend to decrease in typical development and Gross Motor Function Classification System levels I and II groups. However, in low-tone (spinal muscular atrophy types 1 and 2) and high-tone groups (Gross Motor Function Classification System levels IV and V), neck-shaft angle and head-shaft angle tend to increase with age. In both low-tone and high-tone groups, coxa valga is observed. When evaluating the effect of proximal femur-guided growth, these defined normal growth patterns should be considered.</p><p><strong>Level of evidence: </strong>Level III Retrospective comparative study.</p>","PeriodicalId":56060,"journal":{"name":"Journal of Childrens Orthopaedics","volume":"18 5","pages":"523-530"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528760/pdf/","citationCount":"0","resultStr":"{\"title\":\"Femoral neck-shaft angle changes based on the severity of neurologic impairment in children with cerebral palsy and spinal muscular atrophy.\",\"authors\":\"Luiz Carlos Almeida da Silva, Yusuke Hori, Burak Kaymaz, Kenneth J Rogers, Arianna Trionfo, James Richard Bowen, Jason J Howard, Michael Wade Shrader, Freeman Miller\",\"doi\":\"10.1177/18632521241277023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The neck-shaft angle and head-shaft angle in children with varying levels of neurological disability were evaluated to define change over different ages.</p><p><strong>Methods: </strong>Children aged 1-12 years with spastic cerebral palsy, spinal muscular atrophy types 1 and 2, or typical development were reviewed to evaluate the neck-shaft angle and head-shaft angle. Patients were divided into five groups: Gross Motor Function Classification System levels I and II, Gross Motor Function Classification System level III, Gross Motor Function Classification System levels IV and V, spinal muscular atrophy types 1 and 2, and typical development. A linear mixed model was utilized to evaluate neck-shaft angle and head-shaft angle.</p><p><strong>Results: </strong>Data from 196 children (mean age 4.8 ± 4.5 years) were included. Gross Motor Function Classification System levels I and II: 22 children, 130 hip radiographs measured, neck-shaft angle 143.7 ± 7.4, and head-shaft angle 160.0 ± 7.1. Gross Motor Function Classification System level III: 8 children, 33 hips evaluated, neck-shaft angle 153.1 ± 4.3, and head-shaft angle 163.4 ± 4.2. Gross Motor Function Classification System levels IV and V: 30 children, 137 hip radiographs measured, neck-shaft angle 156.4 ± 5.6, and head-shaft angle 167.9 ± 6.8. Spinal muscular atrophy types 1 and 2: 32 children, 83 hip radiographs measured, neck-shaft angle 161.9 ± 9.7, and head-shaft angle 173.4 ± 7.4. Typical development: 104 children, 222 hip radiographs measured, neck-shaft angle 138.6 ± 7.0, and head-shaft angle 156.4 ± 5.9. There were significant statistical differences when comparing neck-shaft angle and head-shaft angle.</p><p><strong>Conclusion: </strong>As children grow, neck-shaft angle and head-shaft angle tend to decrease in typical development and Gross Motor Function Classification System levels I and II groups. However, in low-tone (spinal muscular atrophy types 1 and 2) and high-tone groups (Gross Motor Function Classification System levels IV and V), neck-shaft angle and head-shaft angle tend to increase with age. In both low-tone and high-tone groups, coxa valga is observed. When evaluating the effect of proximal femur-guided growth, these defined normal growth patterns should be considered.</p><p><strong>Level of evidence: </strong>Level III Retrospective comparative study.</p>\",\"PeriodicalId\":56060,\"journal\":{\"name\":\"Journal of Childrens Orthopaedics\",\"volume\":\"18 5\",\"pages\":\"523-530\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528760/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Childrens Orthopaedics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/18632521241277023\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Childrens Orthopaedics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/18632521241277023","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
引言对不同程度神经残疾儿童的颈轴角和头轴角进行评估,以确定不同年龄段的变化:方法:对 1-12 岁患有痉挛性脑瘫、脊髓性肌萎缩症 1 型和 2 型或典型发育的儿童进行复查,以评估颈轴角和头轴角。患者被分为五组:粗大运动功能分级系统 I 级和 II 级组、粗大运动功能分级系统 III 级组、粗大运动功能分级系统 IV 级和 V 级组、脊髓性肌萎缩 1 型和 2 型组以及典型发育组。采用线性混合模型评估颈轴角和头轴角:结果:共纳入了 196 名儿童(平均年龄为 4.8 ± 4.5 岁)的数据。粗大运动功能分级系统 I 级和 II 级:22 名儿童,测量了 130 张髋关节 X 光片,颈轴角为 143.7 ± 7.4,头轴角为 160.0 ± 7.1。粗大运动功能分级系统 III 级:8 名儿童,评估 33 个髋关节,颈轴角为 153.1 ± 4.3,头轴角为 163.4 ± 4.2。粗大运动功能分级系统 IV 级和 V 级:30 名儿童,测量 137 个髋关节 X 光片,颈轴角 156.4 ± 5.6,头轴角 167.9 ± 6.8。脊髓性肌肉萎缩症 1 型和 2 型:32 名儿童,83 张髋关节 X 光片,颈轴角 161.9 ± 9.7,头轴角 173.4 ± 7.4。典型发育:104名儿童,测量222张髋关节X光片,颈轴角为138.6 ± 7.0,头轴角为156.4 ± 5.9。颈轴角和头轴角比较有明显的统计学差异:结论:随着儿童的成长,颈轴角和头轴角在典型发育组和粗大运动功能分级系统 I 级和 II 级组中呈下降趋势。然而,在低音调组(脊髓性肌肉萎缩症 1 型和 2 型)和高音调组(粗大运动功能分类系统 IV 级和 V 级)中,颈轴角和头轴角往往会随着年龄的增长而增大。在低音调组和高音调组中,均可观察到髋臼。在评估股骨近端引导生长的效果时,应考虑这些确定的正常生长模式:证据等级:III 级 回顾性比较研究。
Femoral neck-shaft angle changes based on the severity of neurologic impairment in children with cerebral palsy and spinal muscular atrophy.
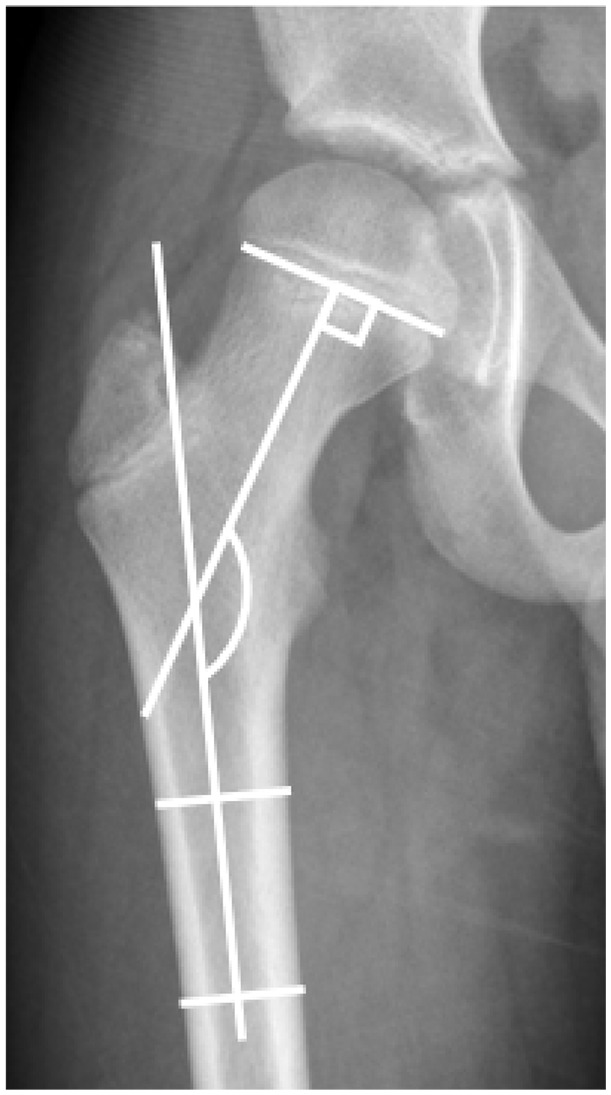
Introduction: The neck-shaft angle and head-shaft angle in children with varying levels of neurological disability were evaluated to define change over different ages.
Methods: Children aged 1-12 years with spastic cerebral palsy, spinal muscular atrophy types 1 and 2, or typical development were reviewed to evaluate the neck-shaft angle and head-shaft angle. Patients were divided into five groups: Gross Motor Function Classification System levels I and II, Gross Motor Function Classification System level III, Gross Motor Function Classification System levels IV and V, spinal muscular atrophy types 1 and 2, and typical development. A linear mixed model was utilized to evaluate neck-shaft angle and head-shaft angle.
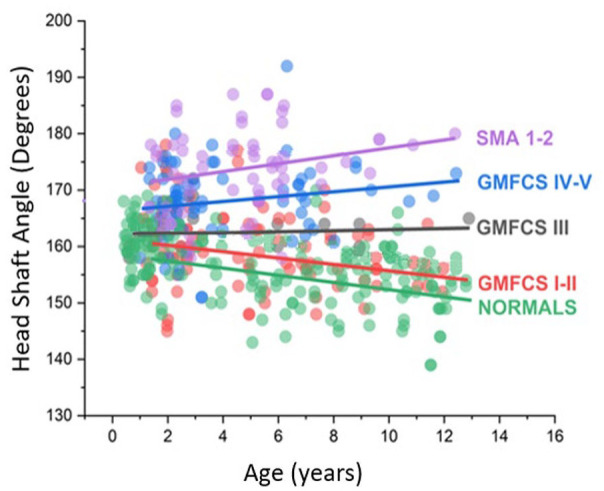
Results: Data from 196 children (mean age 4.8 ± 4.5 years) were included. Gross Motor Function Classification System levels I and II: 22 children, 130 hip radiographs measured, neck-shaft angle 143.7 ± 7.4, and head-shaft angle 160.0 ± 7.1. Gross Motor Function Classification System level III: 8 children, 33 hips evaluated, neck-shaft angle 153.1 ± 4.3, and head-shaft angle 163.4 ± 4.2. Gross Motor Function Classification System levels IV and V: 30 children, 137 hip radiographs measured, neck-shaft angle 156.4 ± 5.6, and head-shaft angle 167.9 ± 6.8. Spinal muscular atrophy types 1 and 2: 32 children, 83 hip radiographs measured, neck-shaft angle 161.9 ± 9.7, and head-shaft angle 173.4 ± 7.4. Typical development: 104 children, 222 hip radiographs measured, neck-shaft angle 138.6 ± 7.0, and head-shaft angle 156.4 ± 5.9. There were significant statistical differences when comparing neck-shaft angle and head-shaft angle.
Conclusion: As children grow, neck-shaft angle and head-shaft angle tend to decrease in typical development and Gross Motor Function Classification System levels I and II groups. However, in low-tone (spinal muscular atrophy types 1 and 2) and high-tone groups (Gross Motor Function Classification System levels IV and V), neck-shaft angle and head-shaft angle tend to increase with age. In both low-tone and high-tone groups, coxa valga is observed. When evaluating the effect of proximal femur-guided growth, these defined normal growth patterns should be considered.
Level of evidence: Level III Retrospective comparative study.
期刊介绍:
Aims & Scope
The Journal of Children’s Orthopaedics is the official journal of the European Paediatric Orthopaedic Society (EPOS) and is published by The British Editorial Society of Bone & Joint Surgery.
It provides a forum for the advancement of the knowledge and education in paediatric orthopaedics and traumatology across geographical borders. It advocates an increased worldwide involvement in preventing and treating musculoskeletal diseases in children and adolescents.
The journal publishes high quality, peer-reviewed articles that focus on clinical practice, diagnosis and treatment of disorders unique to paediatric orthopaedics, as well as on basic and applied research. It aims to help physicians stay abreast of the latest and ever-changing developments in the field of paediatric orthopaedics and traumatology.
The journal welcomes original contributions submitted exclusively for review to the journal. This continuously published online journal is fully open access and will publish one print issue each year to coincide with the EPOS Annual Congress, featuring the meeting’s abstracts.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
