{"title":"模仿甲状旁腺增生的异位宫颈胸腺组织:与巴塞杜氏病有关的罕见病例","authors":"Waralee Chatchomchuan, Yotsapon Thewjitcharoen, Soontaree Nakasatien, Ronnarat Suvikapakornkul, Somboon Keerawat, Thep Himathongkam","doi":"10.1210/jcemcr/luae197","DOIUrl":null,"url":null,"abstract":"<p><p>Thymic hyperplasia has occasionally been reported in patients with Graves disease (GD). However, ectopic cervical thymic hyperplasia in the setting of hyperthyroid GD is exceptionally rare. We describe a case of a 54-year-old Thai woman who presented with hyperthyroidism, diplopia, and pretibial myxedema. She underwent a total thyroidectomy because of diplopia caused by Graves ophthalmopathy. During the surgery, 3 macroscopically abnormal enlargements of parathyroid gland-like tissue were identified and removed. Histopathology revealed hyperplastic thymic tissue mixed with 1 normal-sized parathyroid gland at the location of the left upper parathyroid gland, and thymic tissue was found in the sample labeled as the right upper parathyroid gland. Notably, the sample labeled as the right lower parathyroid gland was actually determined to be a lymph node. Preoperative blood samples showed normal serum calcium and parathyroid hormone levels. Postoperatively, computed tomography of the chest showed thymic hyperplasia in the anterior mediastinum, which slightly regressed at the 9-month follow-up. The patient had transient hypoparathyroidism requiring oral calcium and active vitamin D supplements for 6 months postoperatively. Ectopic cervical thymic hyperplasia can be found in GD and might be indistinguishable from parathyroid hyperplasia. Biochemical evaluations are required to exclude concomitant hyperparathyroidism, and a conservative approach should be considered.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 11","pages":"luae197"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11532649/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ectopic Cervical Thymic Tissue Mimicking Parathyroid Hyperplasia: A Rare Occurrence Linked to Graves Disease.\",\"authors\":\"Waralee Chatchomchuan, Yotsapon Thewjitcharoen, Soontaree Nakasatien, Ronnarat Suvikapakornkul, Somboon Keerawat, Thep Himathongkam\",\"doi\":\"10.1210/jcemcr/luae197\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Thymic hyperplasia has occasionally been reported in patients with Graves disease (GD). However, ectopic cervical thymic hyperplasia in the setting of hyperthyroid GD is exceptionally rare. We describe a case of a 54-year-old Thai woman who presented with hyperthyroidism, diplopia, and pretibial myxedema. She underwent a total thyroidectomy because of diplopia caused by Graves ophthalmopathy. During the surgery, 3 macroscopically abnormal enlargements of parathyroid gland-like tissue were identified and removed. Histopathology revealed hyperplastic thymic tissue mixed with 1 normal-sized parathyroid gland at the location of the left upper parathyroid gland, and thymic tissue was found in the sample labeled as the right upper parathyroid gland. Notably, the sample labeled as the right lower parathyroid gland was actually determined to be a lymph node. Preoperative blood samples showed normal serum calcium and parathyroid hormone levels. Postoperatively, computed tomography of the chest showed thymic hyperplasia in the anterior mediastinum, which slightly regressed at the 9-month follow-up. The patient had transient hypoparathyroidism requiring oral calcium and active vitamin D supplements for 6 months postoperatively. Ectopic cervical thymic hyperplasia can be found in GD and might be indistinguishable from parathyroid hyperplasia. Biochemical evaluations are required to exclude concomitant hyperparathyroidism, and a conservative approach should be considered.</p>\",\"PeriodicalId\":73540,\"journal\":{\"name\":\"JCEM case reports\",\"volume\":\"2 11\",\"pages\":\"luae197\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11532649/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCEM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1210/jcemcr/luae197\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae197","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
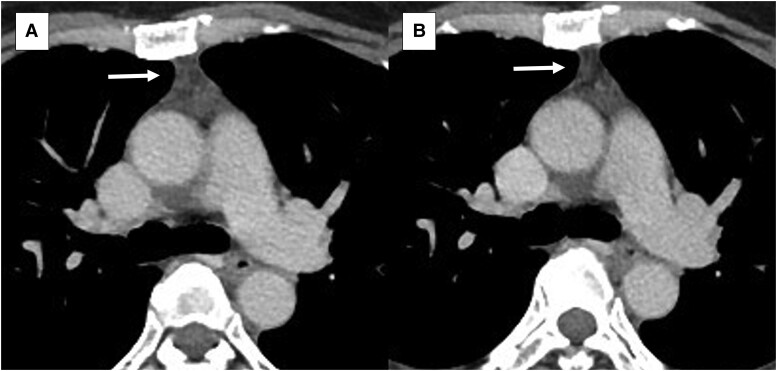
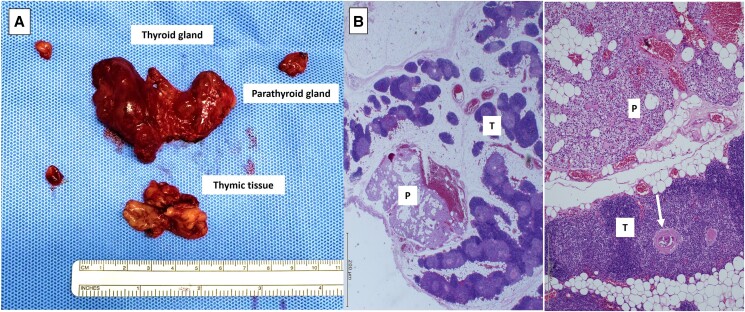
巴塞杜氏病(GD)患者偶尔会出现胸腺增生。然而,甲状腺功能亢进症(GD)患者的异位宫颈胸腺增生异常罕见。我们描述了一例 54 岁的泰国妇女,她出现甲状腺功能亢进、复视和胫前肌水肿。由于巴塞杜氏眼病导致复视,她接受了甲状腺全切除术。手术中发现并切除了3个宏观上异常增大的甲状旁腺样组织。组织病理学检查显示,在左侧甲状旁腺上部的位置,增生的胸腺组织与1个正常大小的甲状旁腺混合在一起,而在标注为右侧甲状旁腺上部的样本中也发现了胸腺组织。值得注意的是,标注为右下甲状旁腺的样本实际上被确定为淋巴结。术前血液样本显示血清钙和甲状旁腺激素水平正常。术后,胸部计算机断层扫描显示前纵隔胸腺增生,9个月随访时略有消退。患者术后出现一过性甲状旁腺功能减退,需要口服钙剂和活性维生素 D 6 个月。异位颈胸腺增生可在广东发现,可能与甲状旁腺增生症无异。需要进行生化评估以排除并发甲状旁腺功能亢进,并应考虑采取保守疗法。
Ectopic Cervical Thymic Tissue Mimicking Parathyroid Hyperplasia: A Rare Occurrence Linked to Graves Disease.
Thymic hyperplasia has occasionally been reported in patients with Graves disease (GD). However, ectopic cervical thymic hyperplasia in the setting of hyperthyroid GD is exceptionally rare. We describe a case of a 54-year-old Thai woman who presented with hyperthyroidism, diplopia, and pretibial myxedema. She underwent a total thyroidectomy because of diplopia caused by Graves ophthalmopathy. During the surgery, 3 macroscopically abnormal enlargements of parathyroid gland-like tissue were identified and removed. Histopathology revealed hyperplastic thymic tissue mixed with 1 normal-sized parathyroid gland at the location of the left upper parathyroid gland, and thymic tissue was found in the sample labeled as the right upper parathyroid gland. Notably, the sample labeled as the right lower parathyroid gland was actually determined to be a lymph node. Preoperative blood samples showed normal serum calcium and parathyroid hormone levels. Postoperatively, computed tomography of the chest showed thymic hyperplasia in the anterior mediastinum, which slightly regressed at the 9-month follow-up. The patient had transient hypoparathyroidism requiring oral calcium and active vitamin D supplements for 6 months postoperatively. Ectopic cervical thymic hyperplasia can be found in GD and might be indistinguishable from parathyroid hyperplasia. Biochemical evaluations are required to exclude concomitant hyperparathyroidism, and a conservative approach should be considered.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
