Philip Y Sun, Kendra Lian, Daniela Markovic, Abdullah Ibish, Roland Faigle, Rebecca Fran Gottesman, Amytis Towfighi
{"title":"急性缺血性脑卒中后住院死亡率的种族/族裔差异。","authors":"Philip Y Sun, Kendra Lian, Daniela Markovic, Abdullah Ibish, Roland Faigle, Rebecca Fran Gottesman, Amytis Towfighi","doi":"10.1159/000542384","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Stroke mortality has declined, with differential changes by race; stroke is now the 5th leading cause of death overall, but 2nd leading cause of death in Black individuals. Little is known about recent race/ethnic and sex trends in in-hospital mortality after acute ischemic stroke (AIS) and whether system-level factors contribute to possible differences.</p><p><strong>Methods: </strong>Using the National Inpatient Sample, adults (≥18 years) with a primary diagnosis of AIS from 2006 to 2017 (n = 643,912) were identified. We assessed in-hospital mortality by race/ethnicity (White, Black, Hispanic, Asian/Pacific Islander [API], other), sex, and age. Hospitals were categorized by proportion of White patients served: \"≥75% White hospitals,\" \"50-75% White hospitals,\" and \"<50% White hospitals.\" Using survey adjusted logistic regression, the association between race/ethnicity and odds of mortality was assessed, adjusting for key sociodemographic, clinical, and hospital characteristics (e.g., age, comorbidities, stroke severity, do not resuscitate orders, and palliative care).</p><p><strong>Results: </strong>Overall, mortality decreased from 5.0% in 2006 to 2.9% in 2017 (p < 0.01). Comparing 2012-2017 to 2006-2011, there was a 68% reduction in mortality odds overall after adjusting for covariates, most prominent in White individuals (69%) and smallest in Black individuals (57%). Compared to White patients, Black and Hispanic patients had lower odds of mortality (adjusted odds ratio [aOR] 0.82, 95% CI 0.78-0.87 and aOR 0.93, 95% CI 0.87-1.00), primarily driven by those >65 years (age × ethnicity interaction p < 0.01). Compared to White men, Black, Hispanic, and API men, and Black women had lower aOR of mortality. The differences in mortality between White and all the other race/ethnic groups combined were most pronounced in ≥75% White hospitals (aOR 0.80, 0.74-0.87) compared to 50-75% White hospitals (aOR 0.85, 0.79-0.91) and <50% White hospitals (aOR 0.88, 0.81-0.95; interaction effect: p < 0.01).</p><p><strong>Conclusion: </strong>AIS mortality has decreased dramatically in recent years in all race/ethnic subgroups. Overall, while individuals of other race/ethnic subgroups had lower mortality odds compared to White individuals, this effect was significantly lower in hospitals serving predominantly White patients compared to those serving minority populations. Further study is needed to understand these differences and to what extent sociocultural, biological, and system-level factors play a role. Category: Health services, quality improvement, and patient-centered outcomes were the elements used to categorize the study sample.</p>","PeriodicalId":9683,"journal":{"name":"Cerebrovascular Diseases","volume":" ","pages":"681-693"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500278/pdf/","citationCount":"0","resultStr":"{\"title\":\"Race/Ethnic Differences in In-Hospital Mortality after Acute Ischemic Stroke.\",\"authors\":\"Philip Y Sun, Kendra Lian, Daniela Markovic, Abdullah Ibish, Roland Faigle, Rebecca Fran Gottesman, Amytis Towfighi\",\"doi\":\"10.1159/000542384\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Stroke mortality has declined, with differential changes by race; stroke is now the 5th leading cause of death overall, but 2nd leading cause of death in Black individuals. Little is known about recent race/ethnic and sex trends in in-hospital mortality after acute ischemic stroke (AIS) and whether system-level factors contribute to possible differences.</p><p><strong>Methods: </strong>Using the National Inpatient Sample, adults (≥18 years) with a primary diagnosis of AIS from 2006 to 2017 (n = 643,912) were identified. We assessed in-hospital mortality by race/ethnicity (White, Black, Hispanic, Asian/Pacific Islander [API], other), sex, and age. Hospitals were categorized by proportion of White patients served: \\\"≥75% White hospitals,\\\" \\\"50-75% White hospitals,\\\" and \\\"<50% White hospitals.\\\" Using survey adjusted logistic regression, the association between race/ethnicity and odds of mortality was assessed, adjusting for key sociodemographic, clinical, and hospital characteristics (e.g., age, comorbidities, stroke severity, do not resuscitate orders, and palliative care).</p><p><strong>Results: </strong>Overall, mortality decreased from 5.0% in 2006 to 2.9% in 2017 (p < 0.01). Comparing 2012-2017 to 2006-2011, there was a 68% reduction in mortality odds overall after adjusting for covariates, most prominent in White individuals (69%) and smallest in Black individuals (57%). Compared to White patients, Black and Hispanic patients had lower odds of mortality (adjusted odds ratio [aOR] 0.82, 95% CI 0.78-0.87 and aOR 0.93, 95% CI 0.87-1.00), primarily driven by those >65 years (age × ethnicity interaction p < 0.01). Compared to White men, Black, Hispanic, and API men, and Black women had lower aOR of mortality. The differences in mortality between White and all the other race/ethnic groups combined were most pronounced in ≥75% White hospitals (aOR 0.80, 0.74-0.87) compared to 50-75% White hospitals (aOR 0.85, 0.79-0.91) and <50% White hospitals (aOR 0.88, 0.81-0.95; interaction effect: p < 0.01).</p><p><strong>Conclusion: </strong>AIS mortality has decreased dramatically in recent years in all race/ethnic subgroups. Overall, while individuals of other race/ethnic subgroups had lower mortality odds compared to White individuals, this effect was significantly lower in hospitals serving predominantly White patients compared to those serving minority populations. Further study is needed to understand these differences and to what extent sociocultural, biological, and system-level factors play a role. Category: Health services, quality improvement, and patient-centered outcomes were the elements used to categorize the study sample.</p>\",\"PeriodicalId\":9683,\"journal\":{\"name\":\"Cerebrovascular Diseases\",\"volume\":\" \",\"pages\":\"681-693\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12500278/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000542384\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000542384","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Race/Ethnic Differences in In-Hospital Mortality after Acute Ischemic Stroke.
Introduction: Stroke mortality has declined, with differential changes by race; stroke is now the 5th leading cause of death overall, but 2nd leading cause of death in Black individuals. Little is known about recent race/ethnic and sex trends in in-hospital mortality after acute ischemic stroke (AIS) and whether system-level factors contribute to possible differences.
Methods: Using the National Inpatient Sample, adults (≥18 years) with a primary diagnosis of AIS from 2006 to 2017 (n = 643,912) were identified. We assessed in-hospital mortality by race/ethnicity (White, Black, Hispanic, Asian/Pacific Islander [API], other), sex, and age. Hospitals were categorized by proportion of White patients served: "≥75% White hospitals," "50-75% White hospitals," and "<50% White hospitals." Using survey adjusted logistic regression, the association between race/ethnicity and odds of mortality was assessed, adjusting for key sociodemographic, clinical, and hospital characteristics (e.g., age, comorbidities, stroke severity, do not resuscitate orders, and palliative care).
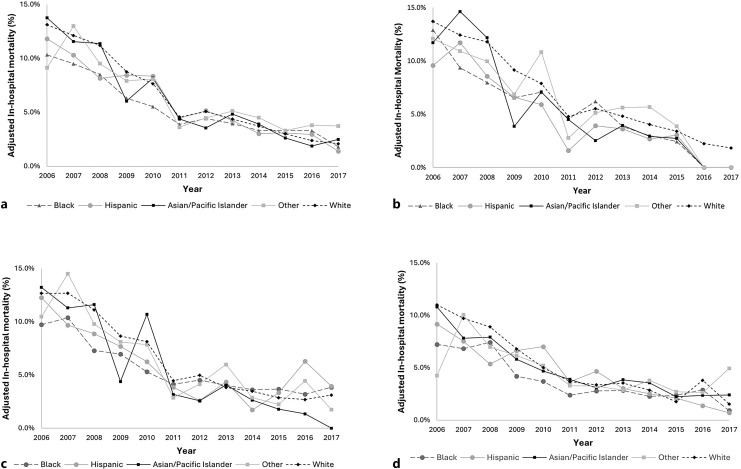
Results: Overall, mortality decreased from 5.0% in 2006 to 2.9% in 2017 (p < 0.01). Comparing 2012-2017 to 2006-2011, there was a 68% reduction in mortality odds overall after adjusting for covariates, most prominent in White individuals (69%) and smallest in Black individuals (57%). Compared to White patients, Black and Hispanic patients had lower odds of mortality (adjusted odds ratio [aOR] 0.82, 95% CI 0.78-0.87 and aOR 0.93, 95% CI 0.87-1.00), primarily driven by those >65 years (age × ethnicity interaction p < 0.01). Compared to White men, Black, Hispanic, and API men, and Black women had lower aOR of mortality. The differences in mortality between White and all the other race/ethnic groups combined were most pronounced in ≥75% White hospitals (aOR 0.80, 0.74-0.87) compared to 50-75% White hospitals (aOR 0.85, 0.79-0.91) and <50% White hospitals (aOR 0.88, 0.81-0.95; interaction effect: p < 0.01).
Conclusion: AIS mortality has decreased dramatically in recent years in all race/ethnic subgroups. Overall, while individuals of other race/ethnic subgroups had lower mortality odds compared to White individuals, this effect was significantly lower in hospitals serving predominantly White patients compared to those serving minority populations. Further study is needed to understand these differences and to what extent sociocultural, biological, and system-level factors play a role. Category: Health services, quality improvement, and patient-centered outcomes were the elements used to categorize the study sample.
期刊介绍:
A rapidly-growing field, stroke and cerebrovascular research is unique in that it involves a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. ''Cerebrovascular Diseases'' is an international forum which meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues, dealing with all aspects of stroke and cerebrovascular diseases. It contains original contributions, reviews of selected topics and clinical investigative studies, recent meeting reports and work-in-progress as well as discussions on controversial issues. All aspects related to clinical advances are considered, while purely experimental work appears if directly relevant to clinical issues.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
