{"title":"对花生过敏的婴幼儿通常也会对树坚果过敏。","authors":"Lara Meixner, Stephanie Heller, Friederike Bluhme, Valérie Trendelenburg, Kirsten Beyer, Birgit Kalb","doi":"10.1002/clt2.70008","DOIUrl":null,"url":null,"abstract":"<p>To the Editor,</p><p>Especially infants with eczema are at high risk for developing food allergies and it is the current understanding that sensitization occurs via the cutaneous route due to an impaired skin barrier function.<span><sup>1, 2</sup></span> Accordingly, a high peanut consumption in the household has been shown to be a possible risk factor for developing peanut allergy in infancy.<span><sup>3</sup></span> Therefore, German S3-guidelines on allergy prevention recommend that peanut allergy should first be ruled out in infants with moderate to severe atopic dermatitis, before introducing peanut into the infant's diet for preventive purposes.<span><sup>4</sup></span> During the last decades, vegan and plant-based diets have become a growing trend.<span><sup>5</sup></span> Tree nuts, such as cashews, hazelnuts and walnuts are a nutritional mainstay of plant-based diets and plant-based alternatives for milk and milk-products often contain tree nuts.<span><sup>5</sup></span> These changes in dietary habits may lead to a wider spread of tree nut allergens in households, increasing the risk for cutaneous exposure. There are hints, that individuals with peanut allergy have a higher likelihood of being allergic to tree nuts compared to the general population.<span><sup>6, 7</sup></span> Therefore, the aim of this study was to investigate how often peanut-sensitized infants and toddlers are sensitized to cashew, hazelnut and walnut as well as their seed storage proteins, which might be associated with a high risk for clinical reactivity.</p><p>The study cohort consists of infants and toddlers who were referred to the Department of Pediatric Respiratory Medicine, Immunology and Critical Care Medicine, Charité—Universitätsmedizin Berlin. Some of the patients underwent an oral food challenge (OFC) for routine diagnostics between 2007 and 2020. Blood as well as clinical data was collected from all patients in the frame of routine diagnostics. Inclusion criteria for the analysis of co-sensitization was age ≤2 years and specific IgE (sIgE) to peanut ≥0.1 kU/l.</p><p>The detection of sIgE to peanut, hazelnut, walnut and cashew and to their respective 2S albumins Ara h 2, Cor a 14, Jug r 1, Ana o 3 as well as to the 7S vicilin-like globulin Ara h 1, was performed by using the NOVEOS<sup>TM</sup> immunoanalyzer (Garden Grove, California, USA). Sensitization was defined as sIgE ≥0.1 kU/l.</p><p>In order to determine the probability for a positive hazelnut food challenge by Cor a 14-sIgE and for a positive cashew food challenge by Ana o 3-sIgE for each patient, probability curves by Beyer et al. and Lange et al. were utilized.<span><sup>8, 9</sup></span> Since there is no probability curve available for walnut, the individual risk for a positive OFC with walnut could not be estimated (see Supporting Information S1 for detailed methods).</p><p>Sera from 101 peanut-sensitized patients (peanut-sIgE ≥0.1 kU/l) were analyzed. The median age of the patients at the time of blood drawing was 16 months (range: 5–24 months). Nearly all patients (98%) suffered from eczema. Details on patient characteristics are provided in Table 1.</p><p>Specific IgE ≥0.1 kU/l to at least one tree nut was detected in 96.0% (<i>n</i> = 97) of the patients. Most children were sensitized to hazelnut (<i>n</i> = 95; 94.1%), followed by walnut (<i>n</i> = 88; 87.1%) and cashew (<i>n</i> = 85; 84.2%). More than a half (59/101; 58.4%) were sensitized to at least one 2S albumin. 42 patients (41.6%) were sensitized to Cor a 14 and Jug r 1, while 40 patients (39.6%) were sensitized to Ana o 3 (sIgE levels are provided in Table 1). We detected sIgE ≥0.1 kU/l to all three tree nuts in 80.2% (<i>n</i> = 81). Furthermore, 26.7% (<i>n</i> = 27) of the children showed sIgE to all of the corresponding 2S albumins. Children sensitized to all three 2S albumins tended to have higher sIgE levels to the extracts than those sensitized to none or one 2S albumin (data not shown). Of the participants aged ≤12 months (<i>n</i> = 26; 25.7%), 88.5% (<i>n</i> = 23) were sensitized to at least one tree nut, 46.2% (<i>n</i> = 12) to at least one 2S albumin and 34.6% (<i>n</i> = 9) to all three 2S albumins (data not shown).</p><p>Five of the 101 peanut-sensitized infants and toddlers (5.0%) would have reacted with 90% probability to hazelnut and 14 (13.9%) to cashew. In total, 15.8% (<i>n</i> = 16) of all peanut-sensitized children had an at least 90% predicted probability to be allergic to hazelnut and/or cashew (Figure 1).</p><p>We were able to show that peanut-sensitized infants and toddlers are often co-sensitized to tree nuts and their 2S albumins. Regarding co-existing tree nut allergy among peanut-allergic children several observational studies showed that peanut allergy is a risk factor for tree nut allergy.<span><sup>6, 7</sup></span> Moreover, our data indicates that even very young peanut-sensitized children with eczema below 2 years of age may frequently be sensitized to tree nuts and their seed storage proteins. Almost all of the children included in our analysis (98%) suffered from eczema, which is known to be a major risk factor for sensitization and the development of food allergy.<span><sup>2</sup></span></p><p>A few limitations of our study have to be mentioned. As this was a retrospective analysis of stored serum samples, we had no data on the clinical relevance of the tree nut sensitization. In particular, we lacked information on whether an oral food challenge had been conducted or what its outcome was. Moreover, the period of study inclusion was relatively long (2007–2020). However, specific recommendations for the early introduction of food allergens (e.g. peanut) for allergy prevention were published after this period.</p><p>In conclusion, our study at a tertiary care clinic demonstrates that a very high proportion of peanut-sensitized infants and toddlers with eczema are already co-sensitized to tree nuts, with a high likelihood for allergic reactions in a considerable proportion of them. Therefore, it should be considered to determine sIgE to tree nuts in peanut-sensitized children if tree nuts have not been consumed so far. In case of a sensitization to tree nuts, an OFC should be performed to determine its clinical relevance.</p><p><b>Lara Meixner</b>: Investigation (equal); formal analysis (lead); validation (equal); writing—original draft (lead); writing—review and editing (equal). <b>Stephanie Heller</b>: Investigation (equal); validation (equal); writing—review and editing (equal). <b>Friederike Bluhme</b>: Investigation (equal); writing—review and editing (equal). <b>Valérie Trendelenburg</b>: Investigation (equal); writing—review and editing (equal). <b>Kirsten Beyer</b>: Conceptualization (equal); formal analysis (supporting); writing—original draft (supporting); writing—review and editing (lead); funding acquisition (equal); supervision (equal). <b>Birgit Kalb</b>: Conceptualization (equal); formal analysis (supporting); writing—original draft (supporting); writing—review and editing (lead); funding acquisition (equal); supervision (equal).</p><p>Kirsten Beyer reports advisory board/consulting fees or speakers bureau from Aimmune Therapeutics, Bencard, Danone/Nutricia, DBV, Hycor, Infectopharm, Mabylon, Meda Pharma/Mylan, Nestle, Novartis and ThermoFisher as well as research grants from Aimmune, ALK, Danone/Nutricia, DBV Technologies, Hipp, Hycor, Infectopharm and Novartis outside the submitted work. Birgit Kalb reports advisory board/consulting fees from Viatris. Valérie Trendelenburg received speaker's fees from Nutricia/Danone. Friederike Bluhme, Stephanie Heller and Lara Meixner have nothing to disclose.</p>","PeriodicalId":10334,"journal":{"name":"Clinical and Translational Allergy","volume":"14 11","pages":""},"PeriodicalIF":4.0000,"publicationDate":"2024-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.70008","citationCount":"0","resultStr":"{\"title\":\"Infants and toddlers with sensitization to peanut are often co-sensitized to tree nuts\",\"authors\":\"Lara Meixner, Stephanie Heller, Friederike Bluhme, Valérie Trendelenburg, Kirsten Beyer, Birgit Kalb\",\"doi\":\"10.1002/clt2.70008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>To the Editor,</p><p>Especially infants with eczema are at high risk for developing food allergies and it is the current understanding that sensitization occurs via the cutaneous route due to an impaired skin barrier function.<span><sup>1, 2</sup></span> Accordingly, a high peanut consumption in the household has been shown to be a possible risk factor for developing peanut allergy in infancy.<span><sup>3</sup></span> Therefore, German S3-guidelines on allergy prevention recommend that peanut allergy should first be ruled out in infants with moderate to severe atopic dermatitis, before introducing peanut into the infant's diet for preventive purposes.<span><sup>4</sup></span> During the last decades, vegan and plant-based diets have become a growing trend.<span><sup>5</sup></span> Tree nuts, such as cashews, hazelnuts and walnuts are a nutritional mainstay of plant-based diets and plant-based alternatives for milk and milk-products often contain tree nuts.<span><sup>5</sup></span> These changes in dietary habits may lead to a wider spread of tree nut allergens in households, increasing the risk for cutaneous exposure. There are hints, that individuals with peanut allergy have a higher likelihood of being allergic to tree nuts compared to the general population.<span><sup>6, 7</sup></span> Therefore, the aim of this study was to investigate how often peanut-sensitized infants and toddlers are sensitized to cashew, hazelnut and walnut as well as their seed storage proteins, which might be associated with a high risk for clinical reactivity.</p><p>The study cohort consists of infants and toddlers who were referred to the Department of Pediatric Respiratory Medicine, Immunology and Critical Care Medicine, Charité—Universitätsmedizin Berlin. Some of the patients underwent an oral food challenge (OFC) for routine diagnostics between 2007 and 2020. Blood as well as clinical data was collected from all patients in the frame of routine diagnostics. Inclusion criteria for the analysis of co-sensitization was age ≤2 years and specific IgE (sIgE) to peanut ≥0.1 kU/l.</p><p>The detection of sIgE to peanut, hazelnut, walnut and cashew and to their respective 2S albumins Ara h 2, Cor a 14, Jug r 1, Ana o 3 as well as to the 7S vicilin-like globulin Ara h 1, was performed by using the NOVEOS<sup>TM</sup> immunoanalyzer (Garden Grove, California, USA). Sensitization was defined as sIgE ≥0.1 kU/l.</p><p>In order to determine the probability for a positive hazelnut food challenge by Cor a 14-sIgE and for a positive cashew food challenge by Ana o 3-sIgE for each patient, probability curves by Beyer et al. and Lange et al. were utilized.<span><sup>8, 9</sup></span> Since there is no probability curve available for walnut, the individual risk for a positive OFC with walnut could not be estimated (see Supporting Information S1 for detailed methods).</p><p>Sera from 101 peanut-sensitized patients (peanut-sIgE ≥0.1 kU/l) were analyzed. The median age of the patients at the time of blood drawing was 16 months (range: 5–24 months). Nearly all patients (98%) suffered from eczema. Details on patient characteristics are provided in Table 1.</p><p>Specific IgE ≥0.1 kU/l to at least one tree nut was detected in 96.0% (<i>n</i> = 97) of the patients. Most children were sensitized to hazelnut (<i>n</i> = 95; 94.1%), followed by walnut (<i>n</i> = 88; 87.1%) and cashew (<i>n</i> = 85; 84.2%). More than a half (59/101; 58.4%) were sensitized to at least one 2S albumin. 42 patients (41.6%) were sensitized to Cor a 14 and Jug r 1, while 40 patients (39.6%) were sensitized to Ana o 3 (sIgE levels are provided in Table 1). We detected sIgE ≥0.1 kU/l to all three tree nuts in 80.2% (<i>n</i> = 81). Furthermore, 26.7% (<i>n</i> = 27) of the children showed sIgE to all of the corresponding 2S albumins. Children sensitized to all three 2S albumins tended to have higher sIgE levels to the extracts than those sensitized to none or one 2S albumin (data not shown). Of the participants aged ≤12 months (<i>n</i> = 26; 25.7%), 88.5% (<i>n</i> = 23) were sensitized to at least one tree nut, 46.2% (<i>n</i> = 12) to at least one 2S albumin and 34.6% (<i>n</i> = 9) to all three 2S albumins (data not shown).</p><p>Five of the 101 peanut-sensitized infants and toddlers (5.0%) would have reacted with 90% probability to hazelnut and 14 (13.9%) to cashew. In total, 15.8% (<i>n</i> = 16) of all peanut-sensitized children had an at least 90% predicted probability to be allergic to hazelnut and/or cashew (Figure 1).</p><p>We were able to show that peanut-sensitized infants and toddlers are often co-sensitized to tree nuts and their 2S albumins. Regarding co-existing tree nut allergy among peanut-allergic children several observational studies showed that peanut allergy is a risk factor for tree nut allergy.<span><sup>6, 7</sup></span> Moreover, our data indicates that even very young peanut-sensitized children with eczema below 2 years of age may frequently be sensitized to tree nuts and their seed storage proteins. Almost all of the children included in our analysis (98%) suffered from eczema, which is known to be a major risk factor for sensitization and the development of food allergy.<span><sup>2</sup></span></p><p>A few limitations of our study have to be mentioned. As this was a retrospective analysis of stored serum samples, we had no data on the clinical relevance of the tree nut sensitization. In particular, we lacked information on whether an oral food challenge had been conducted or what its outcome was. Moreover, the period of study inclusion was relatively long (2007–2020). However, specific recommendations for the early introduction of food allergens (e.g. peanut) for allergy prevention were published after this period.</p><p>In conclusion, our study at a tertiary care clinic demonstrates that a very high proportion of peanut-sensitized infants and toddlers with eczema are already co-sensitized to tree nuts, with a high likelihood for allergic reactions in a considerable proportion of them. Therefore, it should be considered to determine sIgE to tree nuts in peanut-sensitized children if tree nuts have not been consumed so far. In case of a sensitization to tree nuts, an OFC should be performed to determine its clinical relevance.</p><p><b>Lara Meixner</b>: Investigation (equal); formal analysis (lead); validation (equal); writing—original draft (lead); writing—review and editing (equal). <b>Stephanie Heller</b>: Investigation (equal); validation (equal); writing—review and editing (equal). <b>Friederike Bluhme</b>: Investigation (equal); writing—review and editing (equal). <b>Valérie Trendelenburg</b>: Investigation (equal); writing—review and editing (equal). <b>Kirsten Beyer</b>: Conceptualization (equal); formal analysis (supporting); writing—original draft (supporting); writing—review and editing (lead); funding acquisition (equal); supervision (equal). <b>Birgit Kalb</b>: Conceptualization (equal); formal analysis (supporting); writing—original draft (supporting); writing—review and editing (lead); funding acquisition (equal); supervision (equal).</p><p>Kirsten Beyer reports advisory board/consulting fees or speakers bureau from Aimmune Therapeutics, Bencard, Danone/Nutricia, DBV, Hycor, Infectopharm, Mabylon, Meda Pharma/Mylan, Nestle, Novartis and ThermoFisher as well as research grants from Aimmune, ALK, Danone/Nutricia, DBV Technologies, Hipp, Hycor, Infectopharm and Novartis outside the submitted work. Birgit Kalb reports advisory board/consulting fees from Viatris. Valérie Trendelenburg received speaker's fees from Nutricia/Danone. Friederike Bluhme, Stephanie Heller and Lara Meixner have nothing to disclose.</p>\",\"PeriodicalId\":10334,\"journal\":{\"name\":\"Clinical and Translational Allergy\",\"volume\":\"14 11\",\"pages\":\"\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clt2.70008\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clt2.70008\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clt2.70008","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
摘要
致编者,尤其是患有湿疹的婴儿是食物过敏的高危人群,目前的认识是,由于皮肤屏障功能受损,过敏是通过皮肤途径发生的。3 因此,德国关于过敏预防的 S3 指南建议,在将花生引入婴儿饮食以达到预防目的之前,应首先排除患有中度至重度特应性皮炎的婴儿对花生过敏的可能性。5 这些饮食习惯的改变可能会导致树坚果过敏原在家庭中更广泛地传播,增加皮肤接触的风险。有迹象表明,与普通人群相比,花生过敏患者对树坚果过敏的可能性更高、7 因此,本研究旨在调查对花生过敏的婴幼儿对腰果、榛子和核桃及其种子贮藏蛋白过敏的频率,这可能与临床反应性的高风险相关。其中一些患者在 2007 年至 2020 年期间接受了口服食物挑战 (OFC) 的常规诊断。所有患者的血液和临床数据都是在常规诊断框架内收集的。共敏性分析的纳入标准是年龄≤2 岁,花生特异性 IgE(sIgE)≥0.1 kU/l。使用 NOVEOSTM 免疫分析仪(Garden Grove, California, USA)检测对花生、榛子、核桃和腰果及其各自的 2S 白蛋白 Ara h 2、Cor a 14、Jug r 1、Ana o 3 以及 7S 类沧蛋白球蛋白 Ara h 1 的特异性 IgE。为了确定每位患者通过 Cor a 14-sIgE 进行榛子食物挑战和通过 Ana o 3-sIgE 进行腰果食物挑战的阳性概率,采用了 Beyer 等人和 Lange 等人的概率曲线、9 由于没有核桃的概率曲线,因此无法估计核桃 OFC 阳性的个体风险(详细方法见辅助信息 S1)。抽血时患者的中位年龄为 16 个月(范围:5-24 个月)。几乎所有患者(98%)都患有湿疹。96.0%的患者(n = 97)对至少一种树坚果的特异性 IgE ≥0.1 kU/l。大多数儿童对榛子(95 人;94.1%)过敏,其次是核桃(88 人;87.1%)和腰果(85 人;84.2%)。超过一半的患者(59/101;58.4%)对至少一种 2S 白蛋白过敏。42 名患者(41.6%)对 Cor a 14 和 Jug r 1 敏感,40 名患者(39.6%)对 Ana o 3 敏感(sIgE 水平见表 1)。我们检测到 80.2% 的患者(n = 81)对所有三种树坚果的 sIgE ≥0.1 kU/l。此外,26.7% 的儿童(n = 27)对所有相应的 2S 蛋白都显示出了 sIgE。对所有三种 2S 白蛋白都过敏的儿童对提取物的 sIgE 水平往往高于对任何一种或一种 2S 白蛋白都不过敏的儿童(数据未显示)。在年龄小于 12 个月的参与者中(n = 26;25.7%),88.5%(n = 23)对至少一种树坚果过敏,46.2%(n = 12)对至少一种 2S 白蛋白过敏,34.6%(n = 9)对所有三种 2S 白蛋白过敏(数据未显示)。在 101 个对花生过敏的婴幼儿中,5 个(5.0%)对榛子过敏的可能性为 90%,14 个(13.9%)对腰果过敏。在所有对花生过敏的儿童中,共有 15.8%(n = 16)的儿童对榛子和/或腰果过敏的预测概率至少达到 90%(图 1)。关于对花生过敏的儿童同时对树坚果过敏的问题,一些观察性研究表明,花生过敏是导致树坚果过敏的一个危险因素。在我们的分析中,几乎所有儿童(98%)都患有湿疹,而众所周知,湿疹是导致过敏和食物过敏的一个主要风险因素。
Infants and toddlers with sensitization to peanut are often co-sensitized to tree nuts
To the Editor,
Especially infants with eczema are at high risk for developing food allergies and it is the current understanding that sensitization occurs via the cutaneous route due to an impaired skin barrier function.1, 2 Accordingly, a high peanut consumption in the household has been shown to be a possible risk factor for developing peanut allergy in infancy.3 Therefore, German S3-guidelines on allergy prevention recommend that peanut allergy should first be ruled out in infants with moderate to severe atopic dermatitis, before introducing peanut into the infant's diet for preventive purposes.4 During the last decades, vegan and plant-based diets have become a growing trend.5 Tree nuts, such as cashews, hazelnuts and walnuts are a nutritional mainstay of plant-based diets and plant-based alternatives for milk and milk-products often contain tree nuts.5 These changes in dietary habits may lead to a wider spread of tree nut allergens in households, increasing the risk for cutaneous exposure. There are hints, that individuals with peanut allergy have a higher likelihood of being allergic to tree nuts compared to the general population.6, 7 Therefore, the aim of this study was to investigate how often peanut-sensitized infants and toddlers are sensitized to cashew, hazelnut and walnut as well as their seed storage proteins, which might be associated with a high risk for clinical reactivity.
The study cohort consists of infants and toddlers who were referred to the Department of Pediatric Respiratory Medicine, Immunology and Critical Care Medicine, Charité—Universitätsmedizin Berlin. Some of the patients underwent an oral food challenge (OFC) for routine diagnostics between 2007 and 2020. Blood as well as clinical data was collected from all patients in the frame of routine diagnostics. Inclusion criteria for the analysis of co-sensitization was age ≤2 years and specific IgE (sIgE) to peanut ≥0.1 kU/l.
The detection of sIgE to peanut, hazelnut, walnut and cashew and to their respective 2S albumins Ara h 2, Cor a 14, Jug r 1, Ana o 3 as well as to the 7S vicilin-like globulin Ara h 1, was performed by using the NOVEOSTM immunoanalyzer (Garden Grove, California, USA). Sensitization was defined as sIgE ≥0.1 kU/l.
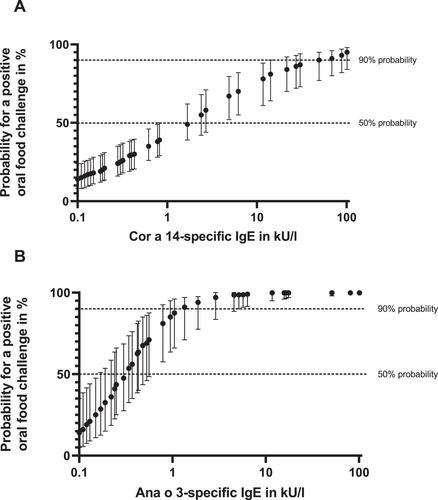
In order to determine the probability for a positive hazelnut food challenge by Cor a 14-sIgE and for a positive cashew food challenge by Ana o 3-sIgE for each patient, probability curves by Beyer et al. and Lange et al. were utilized.8, 9 Since there is no probability curve available for walnut, the individual risk for a positive OFC with walnut could not be estimated (see Supporting Information S1 for detailed methods).
Sera from 101 peanut-sensitized patients (peanut-sIgE ≥0.1 kU/l) were analyzed. The median age of the patients at the time of blood drawing was 16 months (range: 5–24 months). Nearly all patients (98%) suffered from eczema. Details on patient characteristics are provided in Table 1.
Specific IgE ≥0.1 kU/l to at least one tree nut was detected in 96.0% (n = 97) of the patients. Most children were sensitized to hazelnut (n = 95; 94.1%), followed by walnut (n = 88; 87.1%) and cashew (n = 85; 84.2%). More than a half (59/101; 58.4%) were sensitized to at least one 2S albumin. 42 patients (41.6%) were sensitized to Cor a 14 and Jug r 1, while 40 patients (39.6%) were sensitized to Ana o 3 (sIgE levels are provided in Table 1). We detected sIgE ≥0.1 kU/l to all three tree nuts in 80.2% (n = 81). Furthermore, 26.7% (n = 27) of the children showed sIgE to all of the corresponding 2S albumins. Children sensitized to all three 2S albumins tended to have higher sIgE levels to the extracts than those sensitized to none or one 2S albumin (data not shown). Of the participants aged ≤12 months (n = 26; 25.7%), 88.5% (n = 23) were sensitized to at least one tree nut, 46.2% (n = 12) to at least one 2S albumin and 34.6% (n = 9) to all three 2S albumins (data not shown).
Five of the 101 peanut-sensitized infants and toddlers (5.0%) would have reacted with 90% probability to hazelnut and 14 (13.9%) to cashew. In total, 15.8% (n = 16) of all peanut-sensitized children had an at least 90% predicted probability to be allergic to hazelnut and/or cashew (Figure 1).
We were able to show that peanut-sensitized infants and toddlers are often co-sensitized to tree nuts and their 2S albumins. Regarding co-existing tree nut allergy among peanut-allergic children several observational studies showed that peanut allergy is a risk factor for tree nut allergy.6, 7 Moreover, our data indicates that even very young peanut-sensitized children with eczema below 2 years of age may frequently be sensitized to tree nuts and their seed storage proteins. Almost all of the children included in our analysis (98%) suffered from eczema, which is known to be a major risk factor for sensitization and the development of food allergy.2
A few limitations of our study have to be mentioned. As this was a retrospective analysis of stored serum samples, we had no data on the clinical relevance of the tree nut sensitization. In particular, we lacked information on whether an oral food challenge had been conducted or what its outcome was. Moreover, the period of study inclusion was relatively long (2007–2020). However, specific recommendations for the early introduction of food allergens (e.g. peanut) for allergy prevention were published after this period.
In conclusion, our study at a tertiary care clinic demonstrates that a very high proportion of peanut-sensitized infants and toddlers with eczema are already co-sensitized to tree nuts, with a high likelihood for allergic reactions in a considerable proportion of them. Therefore, it should be considered to determine sIgE to tree nuts in peanut-sensitized children if tree nuts have not been consumed so far. In case of a sensitization to tree nuts, an OFC should be performed to determine its clinical relevance.
Kirsten Beyer reports advisory board/consulting fees or speakers bureau from Aimmune Therapeutics, Bencard, Danone/Nutricia, DBV, Hycor, Infectopharm, Mabylon, Meda Pharma/Mylan, Nestle, Novartis and ThermoFisher as well as research grants from Aimmune, ALK, Danone/Nutricia, DBV Technologies, Hipp, Hycor, Infectopharm and Novartis outside the submitted work. Birgit Kalb reports advisory board/consulting fees from Viatris. Valérie Trendelenburg received speaker's fees from Nutricia/Danone. Friederike Bluhme, Stephanie Heller and Lara Meixner have nothing to disclose.
期刊介绍:
Clinical and Translational Allergy, one of several journals in the portfolio of the European Academy of Allergy and Clinical Immunology, provides a platform for the dissemination of allergy research and reviews, as well as EAACI position papers, task force reports and guidelines, amongst an international scientific audience.
Clinical and Translational Allergy accepts clinical and translational research in the following areas and other related topics: asthma, rhinitis, rhinosinusitis, drug hypersensitivity, allergic conjunctivitis, allergic skin diseases, atopic eczema, urticaria, angioedema, venom hypersensitivity, anaphylaxis, food allergy, immunotherapy, immune modulators and biologics, animal models of allergic disease, immune mechanisms, or any other topic related to allergic disease.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
