Sindhuja Kasinathan, Shankar Duraisamy, Rishiraj N Verma
{"title":"视神经鞘直径在预测神经重症患者颅内压升高方面的诊断评估:前瞻性观察研究。","authors":"Sindhuja Kasinathan, Shankar Duraisamy, Rishiraj N Verma","doi":"10.4103/ijciis.ijciis_12_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Optic nerve sheath diameter (ONSD) is used as a surrogate for intracranial pressure (ICP) with a marked variation in its optimal cutoff in various subgroups of neurocritical illnesses. Real-world data on ultrasound (US)-ONSD performance among a diverse population and its trend corresponding with clinical deterioration are scarce. We aim to determine the diagnostic performance of ONSD compared to computed tomography (CT) in predicting elevated ICP in a mixed population of neurocritical patients.</p><p><strong>Methods: </strong>Baseline ONSD measurements (T1) using B-mode US were recorded among eligible patients. Follow-up ONSD (T2) was recorded during clinical deterioration defined by ≥2 drops in Glasgow Coma Scale/Full Outline of UnResponsiveness (GCS/FOUR) scores. Its diagnostic performance in predicting elevated ICP was assessed by comparing it with the concurrently taken CT findings as a reference standard. The difference between the two ONSD measurements was termed delta ONSD.</p><p><strong>Results: </strong>In the final analysis, 129 participants were included. The population comprised traumatic brain injury, stroke (hemorrhagic and ischemic), intracranial space-occupying lesions, and other medical conditions. The optimal ONSD (T2) cutoff of 5.23 mm had a diagnostic accuracy of 80.73% to predict elevated ICP (sensitivity: 82%; specificity: 78%; area under the curve: 0.88; and 95% confidence interval [CI]: 0.819-0.941). Each unit increase in delta ONSD was associated with increased odds of need for surgical intervention (odds ratio [OR]: 3.91; 95% CI: 1.31-12.6, <i>P</i> = 0.017) and death at intensive care unit discharge (OR: 8.24; 95% CI: 1.78-41.15, <i>P</i> = 0.007).</p><p><strong>Conclusions: </strong>ONSD cutoff of 5.23 mm has a good diagnostic accuracy in predicting elevated ICP compared to CT during clinical deterioration. ONSD measurements correlate well with corresponding GCS/FOUR scores.</p>","PeriodicalId":13938,"journal":{"name":"International Journal of Critical Illness and Injury Science","volume":"14 3","pages":"120-128"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11540187/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic evaluation of optic nerve sheath diameter in predicting elevated intracranial pressure among neurocritically ill patients: A prospective observational study.\",\"authors\":\"Sindhuja Kasinathan, Shankar Duraisamy, Rishiraj N Verma\",\"doi\":\"10.4103/ijciis.ijciis_12_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Optic nerve sheath diameter (ONSD) is used as a surrogate for intracranial pressure (ICP) with a marked variation in its optimal cutoff in various subgroups of neurocritical illnesses. Real-world data on ultrasound (US)-ONSD performance among a diverse population and its trend corresponding with clinical deterioration are scarce. We aim to determine the diagnostic performance of ONSD compared to computed tomography (CT) in predicting elevated ICP in a mixed population of neurocritical patients.</p><p><strong>Methods: </strong>Baseline ONSD measurements (T1) using B-mode US were recorded among eligible patients. Follow-up ONSD (T2) was recorded during clinical deterioration defined by ≥2 drops in Glasgow Coma Scale/Full Outline of UnResponsiveness (GCS/FOUR) scores. Its diagnostic performance in predicting elevated ICP was assessed by comparing it with the concurrently taken CT findings as a reference standard. The difference between the two ONSD measurements was termed delta ONSD.</p><p><strong>Results: </strong>In the final analysis, 129 participants were included. The population comprised traumatic brain injury, stroke (hemorrhagic and ischemic), intracranial space-occupying lesions, and other medical conditions. The optimal ONSD (T2) cutoff of 5.23 mm had a diagnostic accuracy of 80.73% to predict elevated ICP (sensitivity: 82%; specificity: 78%; area under the curve: 0.88; and 95% confidence interval [CI]: 0.819-0.941). Each unit increase in delta ONSD was associated with increased odds of need for surgical intervention (odds ratio [OR]: 3.91; 95% CI: 1.31-12.6, <i>P</i> = 0.017) and death at intensive care unit discharge (OR: 8.24; 95% CI: 1.78-41.15, <i>P</i> = 0.007).</p><p><strong>Conclusions: </strong>ONSD cutoff of 5.23 mm has a good diagnostic accuracy in predicting elevated ICP compared to CT during clinical deterioration. ONSD measurements correlate well with corresponding GCS/FOUR scores.</p>\",\"PeriodicalId\":13938,\"journal\":{\"name\":\"International Journal of Critical Illness and Injury Science\",\"volume\":\"14 3\",\"pages\":\"120-128\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11540187/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Critical Illness and Injury Science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ijciis.ijciis_12_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Critical Illness and Injury Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijciis.ijciis_12_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Diagnostic evaluation of optic nerve sheath diameter in predicting elevated intracranial pressure among neurocritically ill patients: A prospective observational study.
Background: Optic nerve sheath diameter (ONSD) is used as a surrogate for intracranial pressure (ICP) with a marked variation in its optimal cutoff in various subgroups of neurocritical illnesses. Real-world data on ultrasound (US)-ONSD performance among a diverse population and its trend corresponding with clinical deterioration are scarce. We aim to determine the diagnostic performance of ONSD compared to computed tomography (CT) in predicting elevated ICP in a mixed population of neurocritical patients.
Methods: Baseline ONSD measurements (T1) using B-mode US were recorded among eligible patients. Follow-up ONSD (T2) was recorded during clinical deterioration defined by ≥2 drops in Glasgow Coma Scale/Full Outline of UnResponsiveness (GCS/FOUR) scores. Its diagnostic performance in predicting elevated ICP was assessed by comparing it with the concurrently taken CT findings as a reference standard. The difference between the two ONSD measurements was termed delta ONSD.
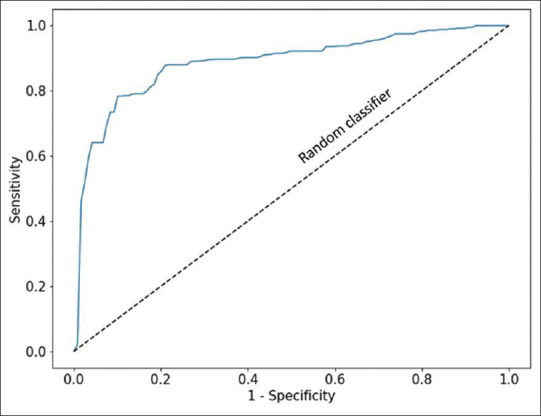
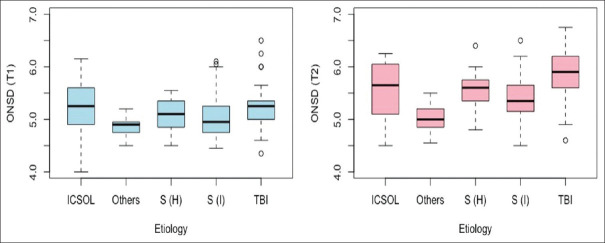
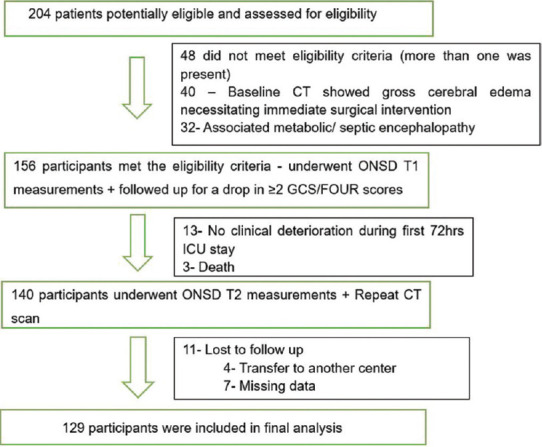
Results: In the final analysis, 129 participants were included. The population comprised traumatic brain injury, stroke (hemorrhagic and ischemic), intracranial space-occupying lesions, and other medical conditions. The optimal ONSD (T2) cutoff of 5.23 mm had a diagnostic accuracy of 80.73% to predict elevated ICP (sensitivity: 82%; specificity: 78%; area under the curve: 0.88; and 95% confidence interval [CI]: 0.819-0.941). Each unit increase in delta ONSD was associated with increased odds of need for surgical intervention (odds ratio [OR]: 3.91; 95% CI: 1.31-12.6, P = 0.017) and death at intensive care unit discharge (OR: 8.24; 95% CI: 1.78-41.15, P = 0.007).
Conclusions: ONSD cutoff of 5.23 mm has a good diagnostic accuracy in predicting elevated ICP compared to CT during clinical deterioration. ONSD measurements correlate well with corresponding GCS/FOUR scores.
期刊介绍:
IJCIIS encourages research, education and dissemination of knowledge in the field of Critical Illness and Injury Science across the world thus promoting translational research by striking a synergy between basic science, clinical medicine and public health. The Journal intends to bring together scientists and academicians in the emergency intensive care and promote translational synergy between Laboratory Science, Clinical Medicine and Public Health. The Journal invites Original Articles, Clinical Investigations, Epidemiological Analysis, Data Protocols, Case Reports, Clinical Photographs, review articles and special commentaries. Students, Residents, Academicians, Public Health experts and scientists are all encouraged to be a part of this initiative by contributing, reviewing and promoting scientific works and science.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
