Ilia Spivak, Atar Lev, Amos J Simon, Ortal Barel, Ido Somekh, Raz Somech
{"title":"一种与综合免疫缺陷和心肌病相关的新型 FNIP1 基因突变。","authors":"Ilia Spivak, Atar Lev, Amos J Simon, Ortal Barel, Ido Somekh, Raz Somech","doi":"10.1007/s00251-024-01359-3","DOIUrl":null,"url":null,"abstract":"<p><p>Genetic variants in Folliculin interacting protein 1 (FNIP1) were recently discovered as monogenic causes for immunodeficiency and cardiomyopathy, with only a few patients diagnosed thus far. In this study, we describe a patient harboring a novel genetic variant in FNIP1 causing immunodeficiency with cardiac involvement. Clinical and immunological workups were performed. Genetic evaluation utilizing whole-exome sequencing (WES) and Sanger sequencing was conducted. The index patient (subject II-4) presented with hypertrophic cardiomyopathy, recurrent infections, and chronic diarrhea during infancy. Immune workup revealed agammaglobulinemia and a lack of B lymphocytes. Genetic evaluation identified a homozygous 13-bp duplication variant in FNIP1 (c.52_64dupGCGCCCGGCCGCG, p. Asp22GlyfsTer21) resulting in a frameshift in exon 1/18. She was treated with supplemental intravenous immunoglobulins (IVIg) with good control of sinopulmonary and gastrointestinal manifestations. Her sibling (subject II-1) had similar clinical features, along with dysmorphic facial features and hypotony, and succumbed to cardiogenic shock at the age of 2 months, prior to genetic evaluation. Diagnosis of novel immunodeficiencies promotes our understanding of the immune system, enabling genetic counseling as herein, and may assist in the development of novel medical therapies in the future. FNIP1 loss-of-function should be considered in patients presenting in infancy with cardiac manifestations along with agammaglobulinemia (and B-cell lymphopenia).</p>","PeriodicalId":13446,"journal":{"name":"Immunogenetics","volume":"77 1","pages":"2"},"PeriodicalIF":2.9000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11561061/pdf/","citationCount":"0","resultStr":"{\"title\":\"A novel mutation in FNIP1 associated with a syndromic immunodeficiency and cardiomyopathy.\",\"authors\":\"Ilia Spivak, Atar Lev, Amos J Simon, Ortal Barel, Ido Somekh, Raz Somech\",\"doi\":\"10.1007/s00251-024-01359-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Genetic variants in Folliculin interacting protein 1 (FNIP1) were recently discovered as monogenic causes for immunodeficiency and cardiomyopathy, with only a few patients diagnosed thus far. In this study, we describe a patient harboring a novel genetic variant in FNIP1 causing immunodeficiency with cardiac involvement. Clinical and immunological workups were performed. Genetic evaluation utilizing whole-exome sequencing (WES) and Sanger sequencing was conducted. The index patient (subject II-4) presented with hypertrophic cardiomyopathy, recurrent infections, and chronic diarrhea during infancy. Immune workup revealed agammaglobulinemia and a lack of B lymphocytes. Genetic evaluation identified a homozygous 13-bp duplication variant in FNIP1 (c.52_64dupGCGCCCGGCCGCG, p. Asp22GlyfsTer21) resulting in a frameshift in exon 1/18. She was treated with supplemental intravenous immunoglobulins (IVIg) with good control of sinopulmonary and gastrointestinal manifestations. Her sibling (subject II-1) had similar clinical features, along with dysmorphic facial features and hypotony, and succumbed to cardiogenic shock at the age of 2 months, prior to genetic evaluation. Diagnosis of novel immunodeficiencies promotes our understanding of the immune system, enabling genetic counseling as herein, and may assist in the development of novel medical therapies in the future. FNIP1 loss-of-function should be considered in patients presenting in infancy with cardiac manifestations along with agammaglobulinemia (and B-cell lymphopenia).</p>\",\"PeriodicalId\":13446,\"journal\":{\"name\":\"Immunogenetics\",\"volume\":\"77 1\",\"pages\":\"2\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11561061/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunogenetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00251-024-01359-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GENETICS & HEREDITY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunogenetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00251-024-01359-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
摘要
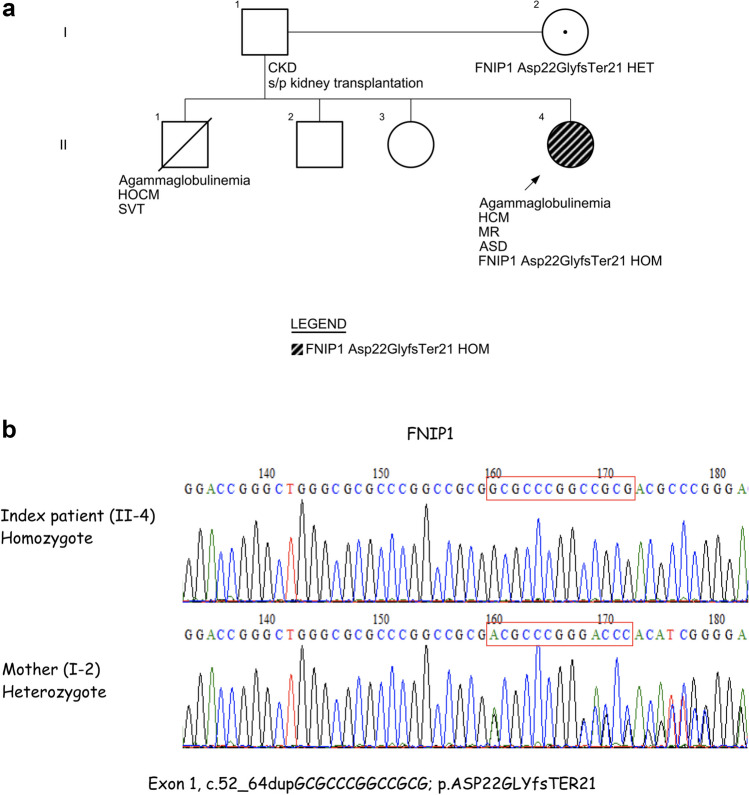
卵泡素互作蛋白 1(FNIP1)的基因变异最近被发现是导致免疫缺陷和心肌病的单基因病因,但迄今只有少数患者被确诊。在本研究中,我们描述了一名携带新型 FNIP1 基因变异的患者,该变异可导致免疫缺陷并累及心脏。我们对该患者进行了临床和免疫学检查。利用全外显子组测序(WES)和桑格测序进行了基因评估。患者(受试者 II-4)在婴儿期出现肥厚型心肌病、反复感染和慢性腹泻。免疫检查结果显示患者患有丙种球蛋白血症并缺乏 B 淋巴细胞。基因评估发现,FNIP1 存在一个 13-bp 的同源重复变异(c.52_64dupGCGCCCGGCCGCG,p. Asp22GlyfsTer21),导致第 1/18 号外显子发生框移位。她接受了静脉补充免疫球蛋白(IVIg)治疗,鼻窦肺和胃肠道症状得到了很好的控制。她的同胞(受试者 II-1)也有类似的临床特征,同时伴有面部畸形和低血压,在接受遗传学评估之前,于 2 个月大时死于心源性休克。新型免疫缺陷的诊断促进了我们对免疫系统的了解,使遗传咨询成为可能,并有助于未来新型医学疗法的开发。在婴儿期出现心脏表现并伴有阿加球蛋白血症(和 B 细胞淋巴细胞减少症)的患者应考虑 FNIP1 功能缺失。
A novel mutation in FNIP1 associated with a syndromic immunodeficiency and cardiomyopathy.
Genetic variants in Folliculin interacting protein 1 (FNIP1) were recently discovered as monogenic causes for immunodeficiency and cardiomyopathy, with only a few patients diagnosed thus far. In this study, we describe a patient harboring a novel genetic variant in FNIP1 causing immunodeficiency with cardiac involvement. Clinical and immunological workups were performed. Genetic evaluation utilizing whole-exome sequencing (WES) and Sanger sequencing was conducted. The index patient (subject II-4) presented with hypertrophic cardiomyopathy, recurrent infections, and chronic diarrhea during infancy. Immune workup revealed agammaglobulinemia and a lack of B lymphocytes. Genetic evaluation identified a homozygous 13-bp duplication variant in FNIP1 (c.52_64dupGCGCCCGGCCGCG, p. Asp22GlyfsTer21) resulting in a frameshift in exon 1/18. She was treated with supplemental intravenous immunoglobulins (IVIg) with good control of sinopulmonary and gastrointestinal manifestations. Her sibling (subject II-1) had similar clinical features, along with dysmorphic facial features and hypotony, and succumbed to cardiogenic shock at the age of 2 months, prior to genetic evaluation. Diagnosis of novel immunodeficiencies promotes our understanding of the immune system, enabling genetic counseling as herein, and may assist in the development of novel medical therapies in the future. FNIP1 loss-of-function should be considered in patients presenting in infancy with cardiac manifestations along with agammaglobulinemia (and B-cell lymphopenia).
期刊介绍:
Immunogenetics publishes original papers, brief communications, and reviews on research in the following areas: genetics and evolution of the immune system; genetic control of immune response and disease susceptibility; bioinformatics of the immune system; structure of immunologically important molecules; and immunogenetics of reproductive biology, tissue differentiation, and development.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
