Zhuyun Cai, Hui Kang, Lei Quan, Yilong Ren, Meng Fang, Yixuan Tan, Haochen Zhang, Xuhui Zhou, Jun Ma
{"title":"颈椎后纵韧带骨化手术治疗的新算法:一项为期两年的回顾性队列研究","authors":"Zhuyun Cai, Hui Kang, Lei Quan, Yilong Ren, Meng Fang, Yixuan Tan, Haochen Zhang, Xuhui Zhou, Jun Ma","doi":"10.1111/os.14293","DOIUrl":null,"url":null,"abstract":"<p><strong>Object: </strong>With the development of new technologies, the surgical algorithm for ossification of posterior longitudinal ligament (OPLL) in the cervical spine also needs to be updated. The aim of this study is to elucidate a new surgical classification algorithm to guide the choice of surgical approaches for cervical OPLL based on its location and extent. In this algorithm, anterior controllable antedisplacement and fusion (ACAF) will be used as a new surgical option.</p><p><strong>Methods: </strong>This is a single-centered, retrospective, cohort study utilizing a novel algorithm based on the following three criteria: (1) the positional relationship between ossification and uncinate process (UP), (2) the K-line, and (3) the ossification segment for surgical decision-making. Patients diagnosed with cervical OPLL who received surgical intervention guided by the algorithm were included. Patient demographics, Japanese Orthopedic Association (JOA) scores, surgical time, imaging data before and 2 years after surgery, and the occurrence of complications were extracted from the database. Paired t-test was used for intragroup comparison, and one-way ANOVA test was used for the intergroup analyses.</p><p><strong>Results: </strong>Based on this novel algorithm, 15 patients with Type I, 8 patients with Type II a, 2 patients with Type II b1, 5 patients with Type II b2 were included. The decision-making for the surgical techniques used in each patient followed the recommendation of the novel algorithm. The postoperative JOA scores of all types of patients improved significantly (p < 0.05), and the invasion rates of vertebral canal had also been significantly reduced (p < 0.05). In terms of restoring cervical curvature, patients with Type I (receiving ACAF) and Type II b2 (receiving laminectomy with instrumented fusion) benefited more from surgery (p < 0.05).</p><p><strong>Conclusion: </strong>A new algorithm guiding the choice of surgical approach for cervical OPLL was validated in a series of 30 patients. Through this analysis, we obtained on their clinical outcomes and complications. ACAF surgery is an ideal choice for Type I patients, with ossification located between UPs, while for patients with ossification exceeding UPs, it is better to perform anterior cervical corpectomy and fusion or posterior surgery.</p>","PeriodicalId":19566,"journal":{"name":"Orthopaedic Surgery","volume":" ","pages":"393-400"},"PeriodicalIF":2.1000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11787990/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel Algorithm for Surgical Management of Cervical Ossification of Posterior Longitudinal Ligament: A Retrospective Cohort Study With 2-Year Follow-Up.\",\"authors\":\"Zhuyun Cai, Hui Kang, Lei Quan, Yilong Ren, Meng Fang, Yixuan Tan, Haochen Zhang, Xuhui Zhou, Jun Ma\",\"doi\":\"10.1111/os.14293\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Object: </strong>With the development of new technologies, the surgical algorithm for ossification of posterior longitudinal ligament (OPLL) in the cervical spine also needs to be updated. The aim of this study is to elucidate a new surgical classification algorithm to guide the choice of surgical approaches for cervical OPLL based on its location and extent. In this algorithm, anterior controllable antedisplacement and fusion (ACAF) will be used as a new surgical option.</p><p><strong>Methods: </strong>This is a single-centered, retrospective, cohort study utilizing a novel algorithm based on the following three criteria: (1) the positional relationship between ossification and uncinate process (UP), (2) the K-line, and (3) the ossification segment for surgical decision-making. Patients diagnosed with cervical OPLL who received surgical intervention guided by the algorithm were included. Patient demographics, Japanese Orthopedic Association (JOA) scores, surgical time, imaging data before and 2 years after surgery, and the occurrence of complications were extracted from the database. Paired t-test was used for intragroup comparison, and one-way ANOVA test was used for the intergroup analyses.</p><p><strong>Results: </strong>Based on this novel algorithm, 15 patients with Type I, 8 patients with Type II a, 2 patients with Type II b1, 5 patients with Type II b2 were included. The decision-making for the surgical techniques used in each patient followed the recommendation of the novel algorithm. The postoperative JOA scores of all types of patients improved significantly (p < 0.05), and the invasion rates of vertebral canal had also been significantly reduced (p < 0.05). In terms of restoring cervical curvature, patients with Type I (receiving ACAF) and Type II b2 (receiving laminectomy with instrumented fusion) benefited more from surgery (p < 0.05).</p><p><strong>Conclusion: </strong>A new algorithm guiding the choice of surgical approach for cervical OPLL was validated in a series of 30 patients. Through this analysis, we obtained on their clinical outcomes and complications. ACAF surgery is an ideal choice for Type I patients, with ossification located between UPs, while for patients with ossification exceeding UPs, it is better to perform anterior cervical corpectomy and fusion or posterior surgery.</p>\",\"PeriodicalId\":19566,\"journal\":{\"name\":\"Orthopaedic Surgery\",\"volume\":\" \",\"pages\":\"393-400\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11787990/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Orthopaedic Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/os.14293\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/os.14293","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:随着新技术的发展,颈椎后纵韧带骨化(OPLL)的手术算法也需要更新。本研究旨在阐明一种新的手术分类算法,以指导根据颈椎后纵韧带骨化的位置和程度选择手术方法。在该算法中,前路可控反移位融合术(ACAF)将作为一种新的手术选择:这是一项以单一中心、回顾性、队列研究为基础的新算法,该算法基于以下三个标准:(方法:这是一项单一中心的回顾性队列研究,利用基于以下三个标准的新算法:(1)骨化与钩突之间的位置关系;(2)K线;(3)骨化节段,以做出手术决策。纳入了在该算法指导下接受手术治疗的确诊为颈椎OPLL的患者。从数据库中提取了患者的人口统计学资料、日本骨科协会(JOA)评分、手术时间、术前和术后两年的影像学数据以及并发症发生情况。组内比较采用配对 t 检验,组间分析采用单因素方差分析:根据这种新算法,共纳入了 15 例 I 型患者、8 例 II a 型患者、2 例 II b1 型患者和 5 例 II b2 型患者。每位患者的手术决策都遵循了新算法的建议。所有类型患者的术后 JOA 评分均有明显改善(P在 30 例患者中验证了指导选择颈椎 OPLL 手术方法的新算法。通过分析,我们了解了他们的临床疗效和并发症。对于骨化位于UPs之间的I型患者,ACAF手术是理想的选择;而对于骨化超过UPs的患者,最好进行颈椎前路椎体后凸融合术或后路手术。
Novel Algorithm for Surgical Management of Cervical Ossification of Posterior Longitudinal Ligament: A Retrospective Cohort Study With 2-Year Follow-Up.
Object: With the development of new technologies, the surgical algorithm for ossification of posterior longitudinal ligament (OPLL) in the cervical spine also needs to be updated. The aim of this study is to elucidate a new surgical classification algorithm to guide the choice of surgical approaches for cervical OPLL based on its location and extent. In this algorithm, anterior controllable antedisplacement and fusion (ACAF) will be used as a new surgical option.
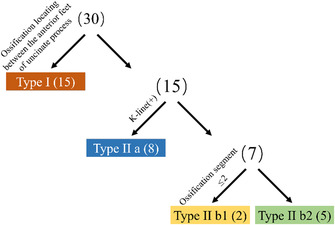
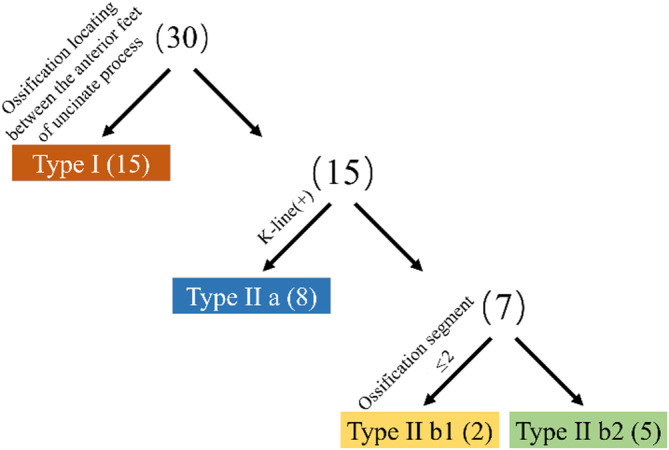
Methods: This is a single-centered, retrospective, cohort study utilizing a novel algorithm based on the following three criteria: (1) the positional relationship between ossification and uncinate process (UP), (2) the K-line, and (3) the ossification segment for surgical decision-making. Patients diagnosed with cervical OPLL who received surgical intervention guided by the algorithm were included. Patient demographics, Japanese Orthopedic Association (JOA) scores, surgical time, imaging data before and 2 years after surgery, and the occurrence of complications were extracted from the database. Paired t-test was used for intragroup comparison, and one-way ANOVA test was used for the intergroup analyses.
Results: Based on this novel algorithm, 15 patients with Type I, 8 patients with Type II a, 2 patients with Type II b1, 5 patients with Type II b2 were included. The decision-making for the surgical techniques used in each patient followed the recommendation of the novel algorithm. The postoperative JOA scores of all types of patients improved significantly (p < 0.05), and the invasion rates of vertebral canal had also been significantly reduced (p < 0.05). In terms of restoring cervical curvature, patients with Type I (receiving ACAF) and Type II b2 (receiving laminectomy with instrumented fusion) benefited more from surgery (p < 0.05).
Conclusion: A new algorithm guiding the choice of surgical approach for cervical OPLL was validated in a series of 30 patients. Through this analysis, we obtained on their clinical outcomes and complications. ACAF surgery is an ideal choice for Type I patients, with ossification located between UPs, while for patients with ossification exceeding UPs, it is better to perform anterior cervical corpectomy and fusion or posterior surgery.
期刊介绍:
Orthopaedic Surgery (OS) is the official journal of the Chinese Orthopaedic Association, focusing on all aspects of orthopaedic technique and surgery.
The journal publishes peer-reviewed articles in the following categories: Original Articles, Clinical Articles, Review Articles, Guidelines, Editorials, Commentaries, Surgical Techniques, Case Reports and Meeting Reports.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
