Sally A. Santen MD PhD, Kimberly Lomis MD, Judee Richardson PhD, John S. Andrews MD, David Henderson MD, Sanjay V. Desai MD
{"title":"精准医学教育:为更好地培养医生以满足患者需求而进行的必要转型。","authors":"Sally A. Santen MD PhD, Kimberly Lomis MD, Judee Richardson PhD, John S. Andrews MD, David Henderson MD, Sanjay V. Desai MD","doi":"10.1002/aet2.11041","DOIUrl":null,"url":null,"abstract":"<p>Across the continuum of emergency medicine (EM) education, physicians strive to continuously develop their skills while navigating multiple demands. To achieve the aim of learning amidst exponential growth in medical knowledge and increasingly complex medical care, a new system of accessible, personalized, and continuous learning is needed. In this commentary, we describe the model of precision medical education (PME),<span><sup>1</sup></span> which includes using data and technology to transform lifelong learning by improving data inputs, personalization, and efficiency.</p><p>Innovation creates transformation in medical education. In other spheres, the arc of innovation empowers users and builds value.<span><sup>2</sup></span> For example, Amazon shifted purchasing power from local stores to consumers.<span><sup>3</sup></span> Netflix transferred power of choice to viewers, creating an industry for asynchronous content. Google shifted power of information from the few to many.<span><sup>4</sup></span> Generative AI (artificial and augmented intelligence) similarly has shifted the ability to gain and apply knowledge from experts to the people. While it takes time to fully realize their potential, these innovations largely meet the needs of consumers and society by shifting the locus of control to the end users. We believe medical education should create similar transformational shifts for learning to bring the locus of control to individual—student, emergency medicine (EM) resident, and practicing physician in the arc of lifelong learning.</p><p>The goal of training is to produce an EM physician workforce capable of delivering high-quality care to patients and communities. Explosive growth in medical knowledge and remarkable procedural advances have underscored physicians’ need for continuous and effective lifelong learning. The need to make this learning simple and accessible so that it weaves within existing workflows is also an imperative. Yet how do physicians maintain and advance their knowledge?<span><sup>5</sup></span> The gap between the need and process of learning, including resources, time, and methods, can contribute to the challenges of ongoing learning, contributing to burnout and moral distress as physicians struggle to keep up.</p><p>Medical education for medical students, residents, and practicing physicians has not evolved sufficiently with the pace of change in technology and remains encumbered by inflexibility, inefficiency, and inequity. This gap enhances the struggle to meet the current and future needs of physicians.<span><sup>6</sup></span> There is little emphasis on the process of lifelong learning or maintaining competency in the rapidly expanding universe of medical knowledge and new procedures.</p><p>Because of resource constraints and the need to deliver training at scale, structured medical education (undergraduate medical education, graduate medical education, and continuing professional development [CPD]) are experienced as “one size fits all.” The same curriculum is delivered to all regardless of context, individual knowledge, or patient care needs. Additionally, CPD orients to hours to complete the session or to obtain recertification versus knowledge or skills needed. It becomes performance of a “check the box” approach with substantial frustration without advancing patient-relevant lifelong learning. The system, trainees, and practicing physicians would all benefit from increasing the effectiveness of learning by increasing personalization, efficiency, and power for the individual physician.</p><p>PME is a system using data and technology to transform lifelong learning through improved personalization, learning efficiency, learner/physician agency, feedback, and ultimately, to improve patient outcomes. Building on the model described by Triola and Burk-Rafel,<span><sup>1, 7</sup></span> Desai et al.<span><sup>1</sup></span> proposed PME involving a process cycle (Figure 1). This cycle builds on the quality improvement cycle of plan–do–study (check)–act and the Master Adaptive Learner model with plan–learn–assess–adjust.<span><sup>8</sup></span> The model can function at the individual, program, or organizational and system level. For the individual physician, PME starts with <i>data input sources</i>—proactive data aggregation will be driven by data gathered from a variety of sources including the electronic health record, patient care outcomes, patient panel data, population data, health care quality measures, physician educational activities, and clinical practice patterns. Identifying disparities in care based on patient characteristics is also important to analyze and include as an input source. For EM residents, data inputs might include assessments, return visits, radiology, antibiotics, and narcotic ordering patterns.</p><p>From the analysis of data, we develop <i>insights</i> and understanding of the knowledge and skills gaps. Informatics will enable personalization by leveraging these multisource inputs into meaningful individualized feedback. Insights might include gaps between individual practice and changing practice guidelines or training gaps (e.g., never performing cricothyrotomy or never diagnosing or treating thyroid storm).</p><p><i>Actions and interventions</i> follow<i>—</i>combining these data with individual characteristics and preferences, just-in-time educational programming from high-quality sources such as published research and guidelines, and benchmarking information, will help guide physicians’ development. Ideally coaching will help interpret feedback and increase participation and personalization. For example, by review of resident patient exposures (gap), specific training focused on these gaps can be implemented.</p><p><i>Outcomes</i> including assessment of learning, physician performance, patient outcomes, and evaluation of interventions will provide outcomes for individual and program-level feedback. All information then feeds back into the cycle to provide data as inputs for additional insights, learning, and improvement. Further, issues of disparities of health care can be observed and addressed through interventions in physicians’ education. This cycle of PME system will promote an adaptive learning<span><sup>7</sup></span> culture and help address the stress of practice and lifelong learning.</p><p>Figures 2 envisions a future context where the system of PME is developed and assisting physicians with lifelong learning and improved patient care. While some of this illustration is in the future, pilots are already being developed in PME and we anticipate that generative AI technologies will accelerate these efforts. Schaye and team<span><sup>9</sup></span> are developing natural language processing to assess and provide feedback to residents on clinical reasoning. This system will review each resident's note and assess it for clinical reasoning, providing that information on a resident dashboard where the resident can link to the specific note in the patient chart and thereby seeing where they might improve. The dashboard will also provide summary data to record improvements in clinical reasoning documentation and will be used as outcomes to further improvement.</p><p>Several EM teams are using EPIC metadata to inform residents and EM programs. EPIC provides “signal data,” which is metadata of how the electronic health record (EHR) is used by providers. For example, reports can be created to document how much time and where time is spent (notes, orders, tracking, disposition, and chart review). Similarly, graphs can show how a resident places most of their orders (individual orders or order sets) and smartphrase/macro usage compared to others in the department. These inputs provide data for providers to help them understand their process of work and efficiencies. From the insights, they can adapt their approach and monitor changes. Similar will need to reorderly, Warm et all are providing residents the outcomes of their patients.<span><sup>10</sup></span> Schauer builidng on this are exploring the relationships of patient outcome measures and the EPIC metadata (user use patterns) such as efficiency, inbox metrics, and workflow. While this work is with internal medicine residents, for EM residents, PME would allow residents and faculty to link efficiency metrics EHR usage, to patient throughput and importantly with patient outcomes. EHR-based nudges are offering timely recommendations and just-in-time resources germane to a patient the resident cared for that day or could receive content-specific resources based on gaps in their in-training examination performance or the clinical reasoning documented in their patient care notes.<span><sup>11</sup></span> Woodworth and team<span><sup>12</sup></span> are building a platform for anesthesia residents that aligns competency development, core knowledge, and patient exposure with learning resources to address gaps.</p><p>Haptics and wearable devices are other sources of data/inputs.<span><sup>13</sup></span> Some programs use real-time location service trackers to collect resident location and how much time they spend in the patients’ room or in the work room.<span><sup>12</sup></span> In surgery there is a burgeoning use of haptics to assessment pressure, force, and hand movements and relate these to patient outcomes.<span><sup>13</sup></span> While developing in surgery, we can see how this approach will be useful for EM procedural skills. For example, Phadnis et al.<span><sup>14</sup></span> report on the use of EM haptic simulators for training of lateral canthotomy and thoracostomy. These novel methods of collecting data will provide additional inputs for precision education and will be able to provide outcomes as well.</p><p>These projects intentionally use data to provide feedback to physicians to adapt their learning and practice and the innovations leverage PME to assist physicians to improve patient care. PME can also operate on the program and organizational level. For example, American Board of Medical Specialties just funded a project to provide automated mapping of visit diagnoses to specialty board clinical domains for enhanced assessment, certification, and precision education that include EM mapping of clinical visits to the EM model of care.<span><sup>15</sup></span> Kern et al.<span><sup>16</sup></span> explored the relationship between number of patients seen and in-training examination scores. Hoxha et al. investigated medical students’ types of clinical encounters in the ED in relationship to Clerkship Directors in Emergency Medicine recommendations.<span><sup>17</sup></span> Similar mapping was done for residents’ patients ICD-10 codes.<span><sup>18</sup></span> These data provide macro and meso level information to tailor education at the program or specialty level. EM trainees, physicians, and education leaders can use these examples to identify sources of data and other PME approaches in their own contexts.</p><p>To accelerate this transformation in lifelong learning through PME, we must take advantage of the acute inflection point of growth in technology and analytics. Most EM programs do not have the necessary data infrastructures, and the transition cost to such systems can be imposing, especially for lower-resourced systems. Technological advances may outpace the effective integration of innovation in the learning environment. As the previous section demonstrated, there are pockets of PME in EM, but the issue is the difficulty scaling due to cost, informatics resources, and technology. As PME innovations are developed they need to be replicable, scalable, and accessible and will require significant resources.</p><p>Furthermore, a culture promoting a growth mindset and competency-based patient-centered education, as well as increasing emphasis on adaptive learning<span><sup>12</sup></span> and coaching, is needed to enable PME. The predominant culture frames learning in a deficit orientation, stunting a growth mindset. An entrenched normative orientation of assessment, coupled with a highly competitive selection process for each next phase of training, inhibits the focus on developmental needs. Branzetti and colleagues<span><sup>19-21</sup></span> have several papers exploring master adaptive learner and adaptive expertise that can help EM promote growth mindset. Leveraging this work, as well as coaching, the use of Individualized learning plans, and other shared resources, will help support PME in EM.<span><sup>22</sup></span> Paying attention to the affective and emotional responses to PME will help effectiveness.</p><p>Finally, additional research will be needed on the effectiveness of a PME system, including specific outcome measures related to learning and performance improvements as well as how and why impacts are or are not occurring. For example, there are concerns that AI may incorporate existing bias, in the outputs. Thus, as PME is developed, exploration using a realist evaluation lens of … what works for whom, when, and in what circumstances, so as to identify how PME is working and possible biases that are created. The goal is to empower current and future work that is ongoing to address current educational system shortcomings through PME.</p><p>In conclusion, PME facilitates moving the power of learning to physicians to maximize the value and effectiveness of education. There are several next steps. First, leaders of health systems and educational programs should invest in systems of PME collaboratively and strategically to leverage resources and impact change more effectively. Second, the EM educational community should explore and expand current PME pilots. Third, data exist in medical education; using these data to drive the PME cycle with insights, action, outcomes supported by coaching, master adaptive learning, and growth mindset will start us on the way. With this transformation, the medical education system will become more personalized, efficient, fair, and effective—and ultimately allow physicians to care for patients, families, and communities more capably.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":37032,"journal":{"name":"AEM Education and Training","volume":"8 6","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2024-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11551623/pdf/","citationCount":"0","resultStr":"{\"title\":\"Precision education in medicine: A necessary transformation to better prepare physicians to meet the needs of their patients\",\"authors\":\"Sally A. Santen MD PhD, Kimberly Lomis MD, Judee Richardson PhD, John S. Andrews MD, David Henderson MD, Sanjay V. Desai MD\",\"doi\":\"10.1002/aet2.11041\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Across the continuum of emergency medicine (EM) education, physicians strive to continuously develop their skills while navigating multiple demands. To achieve the aim of learning amidst exponential growth in medical knowledge and increasingly complex medical care, a new system of accessible, personalized, and continuous learning is needed. In this commentary, we describe the model of precision medical education (PME),<span><sup>1</sup></span> which includes using data and technology to transform lifelong learning by improving data inputs, personalization, and efficiency.</p><p>Innovation creates transformation in medical education. In other spheres, the arc of innovation empowers users and builds value.<span><sup>2</sup></span> For example, Amazon shifted purchasing power from local stores to consumers.<span><sup>3</sup></span> Netflix transferred power of choice to viewers, creating an industry for asynchronous content. Google shifted power of information from the few to many.<span><sup>4</sup></span> Generative AI (artificial and augmented intelligence) similarly has shifted the ability to gain and apply knowledge from experts to the people. While it takes time to fully realize their potential, these innovations largely meet the needs of consumers and society by shifting the locus of control to the end users. We believe medical education should create similar transformational shifts for learning to bring the locus of control to individual—student, emergency medicine (EM) resident, and practicing physician in the arc of lifelong learning.</p><p>The goal of training is to produce an EM physician workforce capable of delivering high-quality care to patients and communities. Explosive growth in medical knowledge and remarkable procedural advances have underscored physicians’ need for continuous and effective lifelong learning. The need to make this learning simple and accessible so that it weaves within existing workflows is also an imperative. Yet how do physicians maintain and advance their knowledge?<span><sup>5</sup></span> The gap between the need and process of learning, including resources, time, and methods, can contribute to the challenges of ongoing learning, contributing to burnout and moral distress as physicians struggle to keep up.</p><p>Medical education for medical students, residents, and practicing physicians has not evolved sufficiently with the pace of change in technology and remains encumbered by inflexibility, inefficiency, and inequity. This gap enhances the struggle to meet the current and future needs of physicians.<span><sup>6</sup></span> There is little emphasis on the process of lifelong learning or maintaining competency in the rapidly expanding universe of medical knowledge and new procedures.</p><p>Because of resource constraints and the need to deliver training at scale, structured medical education (undergraduate medical education, graduate medical education, and continuing professional development [CPD]) are experienced as “one size fits all.” The same curriculum is delivered to all regardless of context, individual knowledge, or patient care needs. Additionally, CPD orients to hours to complete the session or to obtain recertification versus knowledge or skills needed. It becomes performance of a “check the box” approach with substantial frustration without advancing patient-relevant lifelong learning. The system, trainees, and practicing physicians would all benefit from increasing the effectiveness of learning by increasing personalization, efficiency, and power for the individual physician.</p><p>PME is a system using data and technology to transform lifelong learning through improved personalization, learning efficiency, learner/physician agency, feedback, and ultimately, to improve patient outcomes. Building on the model described by Triola and Burk-Rafel,<span><sup>1, 7</sup></span> Desai et al.<span><sup>1</sup></span> proposed PME involving a process cycle (Figure 1). This cycle builds on the quality improvement cycle of plan–do–study (check)–act and the Master Adaptive Learner model with plan–learn–assess–adjust.<span><sup>8</sup></span> The model can function at the individual, program, or organizational and system level. For the individual physician, PME starts with <i>data input sources</i>—proactive data aggregation will be driven by data gathered from a variety of sources including the electronic health record, patient care outcomes, patient panel data, population data, health care quality measures, physician educational activities, and clinical practice patterns. Identifying disparities in care based on patient characteristics is also important to analyze and include as an input source. For EM residents, data inputs might include assessments, return visits, radiology, antibiotics, and narcotic ordering patterns.</p><p>From the analysis of data, we develop <i>insights</i> and understanding of the knowledge and skills gaps. Informatics will enable personalization by leveraging these multisource inputs into meaningful individualized feedback. Insights might include gaps between individual practice and changing practice guidelines or training gaps (e.g., never performing cricothyrotomy or never diagnosing or treating thyroid storm).</p><p><i>Actions and interventions</i> follow<i>—</i>combining these data with individual characteristics and preferences, just-in-time educational programming from high-quality sources such as published research and guidelines, and benchmarking information, will help guide physicians’ development. Ideally coaching will help interpret feedback and increase participation and personalization. For example, by review of resident patient exposures (gap), specific training focused on these gaps can be implemented.</p><p><i>Outcomes</i> including assessment of learning, physician performance, patient outcomes, and evaluation of interventions will provide outcomes for individual and program-level feedback. All information then feeds back into the cycle to provide data as inputs for additional insights, learning, and improvement. Further, issues of disparities of health care can be observed and addressed through interventions in physicians’ education. This cycle of PME system will promote an adaptive learning<span><sup>7</sup></span> culture and help address the stress of practice and lifelong learning.</p><p>Figures 2 envisions a future context where the system of PME is developed and assisting physicians with lifelong learning and improved patient care. While some of this illustration is in the future, pilots are already being developed in PME and we anticipate that generative AI technologies will accelerate these efforts. Schaye and team<span><sup>9</sup></span> are developing natural language processing to assess and provide feedback to residents on clinical reasoning. This system will review each resident's note and assess it for clinical reasoning, providing that information on a resident dashboard where the resident can link to the specific note in the patient chart and thereby seeing where they might improve. The dashboard will also provide summary data to record improvements in clinical reasoning documentation and will be used as outcomes to further improvement.</p><p>Several EM teams are using EPIC metadata to inform residents and EM programs. EPIC provides “signal data,” which is metadata of how the electronic health record (EHR) is used by providers. For example, reports can be created to document how much time and where time is spent (notes, orders, tracking, disposition, and chart review). Similarly, graphs can show how a resident places most of their orders (individual orders or order sets) and smartphrase/macro usage compared to others in the department. These inputs provide data for providers to help them understand their process of work and efficiencies. From the insights, they can adapt their approach and monitor changes. Similar will need to reorderly, Warm et all are providing residents the outcomes of their patients.<span><sup>10</sup></span> Schauer builidng on this are exploring the relationships of patient outcome measures and the EPIC metadata (user use patterns) such as efficiency, inbox metrics, and workflow. While this work is with internal medicine residents, for EM residents, PME would allow residents and faculty to link efficiency metrics EHR usage, to patient throughput and importantly with patient outcomes. EHR-based nudges are offering timely recommendations and just-in-time resources germane to a patient the resident cared for that day or could receive content-specific resources based on gaps in their in-training examination performance or the clinical reasoning documented in their patient care notes.<span><sup>11</sup></span> Woodworth and team<span><sup>12</sup></span> are building a platform for anesthesia residents that aligns competency development, core knowledge, and patient exposure with learning resources to address gaps.</p><p>Haptics and wearable devices are other sources of data/inputs.<span><sup>13</sup></span> Some programs use real-time location service trackers to collect resident location and how much time they spend in the patients’ room or in the work room.<span><sup>12</sup></span> In surgery there is a burgeoning use of haptics to assessment pressure, force, and hand movements and relate these to patient outcomes.<span><sup>13</sup></span> While developing in surgery, we can see how this approach will be useful for EM procedural skills. For example, Phadnis et al.<span><sup>14</sup></span> report on the use of EM haptic simulators for training of lateral canthotomy and thoracostomy. These novel methods of collecting data will provide additional inputs for precision education and will be able to provide outcomes as well.</p><p>These projects intentionally use data to provide feedback to physicians to adapt their learning and practice and the innovations leverage PME to assist physicians to improve patient care. PME can also operate on the program and organizational level. For example, American Board of Medical Specialties just funded a project to provide automated mapping of visit diagnoses to specialty board clinical domains for enhanced assessment, certification, and precision education that include EM mapping of clinical visits to the EM model of care.<span><sup>15</sup></span> Kern et al.<span><sup>16</sup></span> explored the relationship between number of patients seen and in-training examination scores. Hoxha et al. investigated medical students’ types of clinical encounters in the ED in relationship to Clerkship Directors in Emergency Medicine recommendations.<span><sup>17</sup></span> Similar mapping was done for residents’ patients ICD-10 codes.<span><sup>18</sup></span> These data provide macro and meso level information to tailor education at the program or specialty level. EM trainees, physicians, and education leaders can use these examples to identify sources of data and other PME approaches in their own contexts.</p><p>To accelerate this transformation in lifelong learning through PME, we must take advantage of the acute inflection point of growth in technology and analytics. Most EM programs do not have the necessary data infrastructures, and the transition cost to such systems can be imposing, especially for lower-resourced systems. Technological advances may outpace the effective integration of innovation in the learning environment. As the previous section demonstrated, there are pockets of PME in EM, but the issue is the difficulty scaling due to cost, informatics resources, and technology. As PME innovations are developed they need to be replicable, scalable, and accessible and will require significant resources.</p><p>Furthermore, a culture promoting a growth mindset and competency-based patient-centered education, as well as increasing emphasis on adaptive learning<span><sup>12</sup></span> and coaching, is needed to enable PME. The predominant culture frames learning in a deficit orientation, stunting a growth mindset. An entrenched normative orientation of assessment, coupled with a highly competitive selection process for each next phase of training, inhibits the focus on developmental needs. Branzetti and colleagues<span><sup>19-21</sup></span> have several papers exploring master adaptive learner and adaptive expertise that can help EM promote growth mindset. Leveraging this work, as well as coaching, the use of Individualized learning plans, and other shared resources, will help support PME in EM.<span><sup>22</sup></span> Paying attention to the affective and emotional responses to PME will help effectiveness.</p><p>Finally, additional research will be needed on the effectiveness of a PME system, including specific outcome measures related to learning and performance improvements as well as how and why impacts are or are not occurring. For example, there are concerns that AI may incorporate existing bias, in the outputs. Thus, as PME is developed, exploration using a realist evaluation lens of … what works for whom, when, and in what circumstances, so as to identify how PME is working and possible biases that are created. The goal is to empower current and future work that is ongoing to address current educational system shortcomings through PME.</p><p>In conclusion, PME facilitates moving the power of learning to physicians to maximize the value and effectiveness of education. There are several next steps. First, leaders of health systems and educational programs should invest in systems of PME collaboratively and strategically to leverage resources and impact change more effectively. Second, the EM educational community should explore and expand current PME pilots. Third, data exist in medical education; using these data to drive the PME cycle with insights, action, outcomes supported by coaching, master adaptive learning, and growth mindset will start us on the way. With this transformation, the medical education system will become more personalized, efficient, fair, and effective—and ultimately allow physicians to care for patients, families, and communities more capably.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":37032,\"journal\":{\"name\":\"AEM Education and Training\",\"volume\":\"8 6\",\"pages\":\"\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-11-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11551623/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AEM Education and Training\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aet2.11041\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EDUCATION, SCIENTIFIC DISCIPLINES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AEM Education and Training","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aet2.11041","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EDUCATION, SCIENTIFIC DISCIPLINES","Score":null,"Total":0}
引用次数: 0
摘要
接下来的行动和干预措施--将这些数据与个人特征和偏好、来自高质量来源(如已发表的研究和指南)的及时教育计划以及基准信息相结合,将有助于指导医生的发展。理想情况下,辅导将有助于解释反馈信息,提高参与度和个性化程度。例如,通过审查住院医师接触病人的情况(差距),可以针对这些差距实施具体的培训。包括学习评估、医师表现、病人结果和干预评估在内的结果将为个人和项目层面的反馈提供结果。然后,所有信息都会反馈到循环中,为更多的见解、学习和改进提供数据作为输入。此外,还可以通过对医生教育的干预来观察和解决医疗差距问题。图 2 构想了一个未来的环境,在这个环境中,继续医学教育系统得到发展,并帮助医生进行终身学习和改善病人护理。虽然其中一些图示还在未来,但 PME 的试点工作已经开始,我们预计生成式人工智能技术将加速这些努力。Schaye 和团队9 正在开发自然语言处理技术,用于评估住院医师的临床推理能力并提供反馈。该系统将审查每位住院医师的病历,并评估其临床推理能力,在住院医师仪表板上提供相关信息,住院医师可通过该仪表板链接到病历中的具体病历,从而了解自己在哪些方面可以改进。仪表板还将提供汇总数据,记录临床推理记录的改进情况,并将其作为进一步改进的成果。一些急诊团队正在使用 EPIC 元数据为住院医师和急诊项目提供信息。EPIC 提供 "信号数据",即医疗服务提供者如何使用电子病历 (EHR) 的元数据。例如,可以创建报告来记录所花费的时间和地点(笔记、医嘱、追踪、处置和病历审查)。同样,图表可以显示住院患者如何下达他们的大部分医嘱(单个医嘱或医嘱集),以及与科室其他人相比的智能短语/宏使用情况。这些输入可为医疗服务提供者提供数据,帮助他们了解自己的工作流程和效率。从这些洞察中,他们可以调整自己的方法并监控变化。在此基础上,Schauer 正在探索患者疗效指标与 EPIC 元数据(用户使用模式)之间的关系,如效率、收件箱指标和工作流程。虽然这项工作的对象是内科住院医师,但对急诊科住院医师而言,PME 可使住院医师和教师将电子病历的使用效率指标与病人吞吐量联系起来,更重要的是与病人预后联系起来。11 Woodworth 和团队12 正在为麻醉住院医师建立一个平台,将能力发展、核心知识和患者接触与学习资源结合起来,以弥补差距。一些项目使用实时定位服务跟踪器来收集住院医生的位置以及他们在病房或工作间花费的时间。例如,Phadnis 等人14 报道了使用电磁触觉模拟器进行外侧犬齿切开术和胸廓切开术培训的情况。这些项目有意利用数据向医生提供反馈,以调整他们的学习和实践,这些创新利用了 PME 来帮助医生改善病人护理。公共教育部也可以在项目和组织层面开展工作。例如,美国医学专科委员会(American Board of Medical Specialties)刚刚资助了一个项目,将就诊诊断自动映射到专科委员会的临床领域,以加强评估、认证和精准教育,其中包括将临床就诊映射到 EM 护理模式。
Precision education in medicine: A necessary transformation to better prepare physicians to meet the needs of their patients
Across the continuum of emergency medicine (EM) education, physicians strive to continuously develop their skills while navigating multiple demands. To achieve the aim of learning amidst exponential growth in medical knowledge and increasingly complex medical care, a new system of accessible, personalized, and continuous learning is needed. In this commentary, we describe the model of precision medical education (PME),1 which includes using data and technology to transform lifelong learning by improving data inputs, personalization, and efficiency.
Innovation creates transformation in medical education. In other spheres, the arc of innovation empowers users and builds value.2 For example, Amazon shifted purchasing power from local stores to consumers.3 Netflix transferred power of choice to viewers, creating an industry for asynchronous content. Google shifted power of information from the few to many.4 Generative AI (artificial and augmented intelligence) similarly has shifted the ability to gain and apply knowledge from experts to the people. While it takes time to fully realize their potential, these innovations largely meet the needs of consumers and society by shifting the locus of control to the end users. We believe medical education should create similar transformational shifts for learning to bring the locus of control to individual—student, emergency medicine (EM) resident, and practicing physician in the arc of lifelong learning.
The goal of training is to produce an EM physician workforce capable of delivering high-quality care to patients and communities. Explosive growth in medical knowledge and remarkable procedural advances have underscored physicians’ need for continuous and effective lifelong learning. The need to make this learning simple and accessible so that it weaves within existing workflows is also an imperative. Yet how do physicians maintain and advance their knowledge?5 The gap between the need and process of learning, including resources, time, and methods, can contribute to the challenges of ongoing learning, contributing to burnout and moral distress as physicians struggle to keep up.
Medical education for medical students, residents, and practicing physicians has not evolved sufficiently with the pace of change in technology and remains encumbered by inflexibility, inefficiency, and inequity. This gap enhances the struggle to meet the current and future needs of physicians.6 There is little emphasis on the process of lifelong learning or maintaining competency in the rapidly expanding universe of medical knowledge and new procedures.
Because of resource constraints and the need to deliver training at scale, structured medical education (undergraduate medical education, graduate medical education, and continuing professional development [CPD]) are experienced as “one size fits all.” The same curriculum is delivered to all regardless of context, individual knowledge, or patient care needs. Additionally, CPD orients to hours to complete the session or to obtain recertification versus knowledge or skills needed. It becomes performance of a “check the box” approach with substantial frustration without advancing patient-relevant lifelong learning. The system, trainees, and practicing physicians would all benefit from increasing the effectiveness of learning by increasing personalization, efficiency, and power for the individual physician.
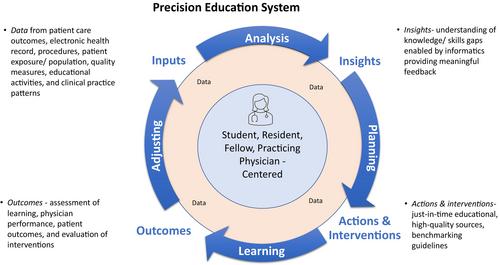
PME is a system using data and technology to transform lifelong learning through improved personalization, learning efficiency, learner/physician agency, feedback, and ultimately, to improve patient outcomes. Building on the model described by Triola and Burk-Rafel,1, 7 Desai et al.1 proposed PME involving a process cycle (Figure 1). This cycle builds on the quality improvement cycle of plan–do–study (check)–act and the Master Adaptive Learner model with plan–learn–assess–adjust.8 The model can function at the individual, program, or organizational and system level. For the individual physician, PME starts with data input sources—proactive data aggregation will be driven by data gathered from a variety of sources including the electronic health record, patient care outcomes, patient panel data, population data, health care quality measures, physician educational activities, and clinical practice patterns. Identifying disparities in care based on patient characteristics is also important to analyze and include as an input source. For EM residents, data inputs might include assessments, return visits, radiology, antibiotics, and narcotic ordering patterns.
From the analysis of data, we develop insights and understanding of the knowledge and skills gaps. Informatics will enable personalization by leveraging these multisource inputs into meaningful individualized feedback. Insights might include gaps between individual practice and changing practice guidelines or training gaps (e.g., never performing cricothyrotomy or never diagnosing or treating thyroid storm).
Actions and interventions follow—combining these data with individual characteristics and preferences, just-in-time educational programming from high-quality sources such as published research and guidelines, and benchmarking information, will help guide physicians’ development. Ideally coaching will help interpret feedback and increase participation and personalization. For example, by review of resident patient exposures (gap), specific training focused on these gaps can be implemented.
Outcomes including assessment of learning, physician performance, patient outcomes, and evaluation of interventions will provide outcomes for individual and program-level feedback. All information then feeds back into the cycle to provide data as inputs for additional insights, learning, and improvement. Further, issues of disparities of health care can be observed and addressed through interventions in physicians’ education. This cycle of PME system will promote an adaptive learning7 culture and help address the stress of practice and lifelong learning.
Figures 2 envisions a future context where the system of PME is developed and assisting physicians with lifelong learning and improved patient care. While some of this illustration is in the future, pilots are already being developed in PME and we anticipate that generative AI technologies will accelerate these efforts. Schaye and team9 are developing natural language processing to assess and provide feedback to residents on clinical reasoning. This system will review each resident's note and assess it for clinical reasoning, providing that information on a resident dashboard where the resident can link to the specific note in the patient chart and thereby seeing where they might improve. The dashboard will also provide summary data to record improvements in clinical reasoning documentation and will be used as outcomes to further improvement.
Several EM teams are using EPIC metadata to inform residents and EM programs. EPIC provides “signal data,” which is metadata of how the electronic health record (EHR) is used by providers. For example, reports can be created to document how much time and where time is spent (notes, orders, tracking, disposition, and chart review). Similarly, graphs can show how a resident places most of their orders (individual orders or order sets) and smartphrase/macro usage compared to others in the department. These inputs provide data for providers to help them understand their process of work and efficiencies. From the insights, they can adapt their approach and monitor changes. Similar will need to reorderly, Warm et all are providing residents the outcomes of their patients.10 Schauer builidng on this are exploring the relationships of patient outcome measures and the EPIC metadata (user use patterns) such as efficiency, inbox metrics, and workflow. While this work is with internal medicine residents, for EM residents, PME would allow residents and faculty to link efficiency metrics EHR usage, to patient throughput and importantly with patient outcomes. EHR-based nudges are offering timely recommendations and just-in-time resources germane to a patient the resident cared for that day or could receive content-specific resources based on gaps in their in-training examination performance or the clinical reasoning documented in their patient care notes.11 Woodworth and team12 are building a platform for anesthesia residents that aligns competency development, core knowledge, and patient exposure with learning resources to address gaps.
Haptics and wearable devices are other sources of data/inputs.13 Some programs use real-time location service trackers to collect resident location and how much time they spend in the patients’ room or in the work room.12 In surgery there is a burgeoning use of haptics to assessment pressure, force, and hand movements and relate these to patient outcomes.13 While developing in surgery, we can see how this approach will be useful for EM procedural skills. For example, Phadnis et al.14 report on the use of EM haptic simulators for training of lateral canthotomy and thoracostomy. These novel methods of collecting data will provide additional inputs for precision education and will be able to provide outcomes as well.
These projects intentionally use data to provide feedback to physicians to adapt their learning and practice and the innovations leverage PME to assist physicians to improve patient care. PME can also operate on the program and organizational level. For example, American Board of Medical Specialties just funded a project to provide automated mapping of visit diagnoses to specialty board clinical domains for enhanced assessment, certification, and precision education that include EM mapping of clinical visits to the EM model of care.15 Kern et al.16 explored the relationship between number of patients seen and in-training examination scores. Hoxha et al. investigated medical students’ types of clinical encounters in the ED in relationship to Clerkship Directors in Emergency Medicine recommendations.17 Similar mapping was done for residents’ patients ICD-10 codes.18 These data provide macro and meso level information to tailor education at the program or specialty level. EM trainees, physicians, and education leaders can use these examples to identify sources of data and other PME approaches in their own contexts.
To accelerate this transformation in lifelong learning through PME, we must take advantage of the acute inflection point of growth in technology and analytics. Most EM programs do not have the necessary data infrastructures, and the transition cost to such systems can be imposing, especially for lower-resourced systems. Technological advances may outpace the effective integration of innovation in the learning environment. As the previous section demonstrated, there are pockets of PME in EM, but the issue is the difficulty scaling due to cost, informatics resources, and technology. As PME innovations are developed they need to be replicable, scalable, and accessible and will require significant resources.
Furthermore, a culture promoting a growth mindset and competency-based patient-centered education, as well as increasing emphasis on adaptive learning12 and coaching, is needed to enable PME. The predominant culture frames learning in a deficit orientation, stunting a growth mindset. An entrenched normative orientation of assessment, coupled with a highly competitive selection process for each next phase of training, inhibits the focus on developmental needs. Branzetti and colleagues19-21 have several papers exploring master adaptive learner and adaptive expertise that can help EM promote growth mindset. Leveraging this work, as well as coaching, the use of Individualized learning plans, and other shared resources, will help support PME in EM.22 Paying attention to the affective and emotional responses to PME will help effectiveness.
Finally, additional research will be needed on the effectiveness of a PME system, including specific outcome measures related to learning and performance improvements as well as how and why impacts are or are not occurring. For example, there are concerns that AI may incorporate existing bias, in the outputs. Thus, as PME is developed, exploration using a realist evaluation lens of … what works for whom, when, and in what circumstances, so as to identify how PME is working and possible biases that are created. The goal is to empower current and future work that is ongoing to address current educational system shortcomings through PME.
In conclusion, PME facilitates moving the power of learning to physicians to maximize the value and effectiveness of education. There are several next steps. First, leaders of health systems and educational programs should invest in systems of PME collaboratively and strategically to leverage resources and impact change more effectively. Second, the EM educational community should explore and expand current PME pilots. Third, data exist in medical education; using these data to drive the PME cycle with insights, action, outcomes supported by coaching, master adaptive learning, and growth mindset will start us on the way. With this transformation, the medical education system will become more personalized, efficient, fair, and effective—and ultimately allow physicians to care for patients, families, and communities more capably.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
