José Paz-Ibarra, Marcio Concepción-Zavaleta, Juan Eduardo Quiroz-Aldave, José Somocurcio-Peralta, María Belén Tite Haro, Paola Solis-Pazmino
{"title":"淀粉样变性甲状腺肿:秘鲁病例系列","authors":"José Paz-Ibarra, Marcio Concepción-Zavaleta, Juan Eduardo Quiroz-Aldave, José Somocurcio-Peralta, María Belén Tite Haro, Paola Solis-Pazmino","doi":"10.17925/EE.2024.20.2.16","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: Amyloid goiter (AG) is a rare cause of thyroid swelling, characterized by deposits of amyloid protein in the thyroid tissue. It can be associated with primary or secondary amyloidosis. Its prevalence in multinodular goiter cases is 0.17%, with rare clinical detection before surgery. <b>Case series:</b> This Peruvian case series comprised three female patients and one male patient, with ages ranging from 28 to 65 years. All individuals had pre-existing inflammatory diseases and reported symptoms including dyspnoea, dysphagia and dysphonia. Upon physical examination, all patients exhibited a grade III goiter. Fine-needle aspiration reported colloid goiter. Three out of the four patients underwent total thyroidectomy and histochemistry revealed AG with positive Congo red staining. <b>Discussion:</b> AG is an uncommon clinical entity. It has been reported to occur more frequently in males, with an average age of diagnosis of 40 years. In our series, we observed a broad age range of patients receiving diagnoses, spanning from 28 to 65 years, with a predominance in females. The consideration of AG should be extended to every patient with an underlying chronic systemic inflammatory disease, especially end stage renal disease. In this context, AG should be included in the differential diagnosis for patients with multinodular goiter exhibiting progressive growth and causing compressive symptoms at the cervical level without affecting thyroid function, as demonstrated in our series. <b>Conclusion:</b> AG, a rare condition, warrants suspicion in the presence of a giant goiter with an underlying systemic inflammatory disease.</p>","PeriodicalId":75231,"journal":{"name":"TouchREVIEWS in endocrinology","volume":"20 2","pages":"124-129"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11548356/pdf/","citationCount":"0","resultStr":"{\"title\":\"Amyloid Goiter: A Peruvian Case Series.\",\"authors\":\"José Paz-Ibarra, Marcio Concepción-Zavaleta, Juan Eduardo Quiroz-Aldave, José Somocurcio-Peralta, María Belén Tite Haro, Paola Solis-Pazmino\",\"doi\":\"10.17925/EE.2024.20.2.16\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b>: Amyloid goiter (AG) is a rare cause of thyroid swelling, characterized by deposits of amyloid protein in the thyroid tissue. It can be associated with primary or secondary amyloidosis. Its prevalence in multinodular goiter cases is 0.17%, with rare clinical detection before surgery. <b>Case series:</b> This Peruvian case series comprised three female patients and one male patient, with ages ranging from 28 to 65 years. All individuals had pre-existing inflammatory diseases and reported symptoms including dyspnoea, dysphagia and dysphonia. Upon physical examination, all patients exhibited a grade III goiter. Fine-needle aspiration reported colloid goiter. Three out of the four patients underwent total thyroidectomy and histochemistry revealed AG with positive Congo red staining. <b>Discussion:</b> AG is an uncommon clinical entity. It has been reported to occur more frequently in males, with an average age of diagnosis of 40 years. In our series, we observed a broad age range of patients receiving diagnoses, spanning from 28 to 65 years, with a predominance in females. The consideration of AG should be extended to every patient with an underlying chronic systemic inflammatory disease, especially end stage renal disease. In this context, AG should be included in the differential diagnosis for patients with multinodular goiter exhibiting progressive growth and causing compressive symptoms at the cervical level without affecting thyroid function, as demonstrated in our series. <b>Conclusion:</b> AG, a rare condition, warrants suspicion in the presence of a giant goiter with an underlying systemic inflammatory disease.</p>\",\"PeriodicalId\":75231,\"journal\":{\"name\":\"TouchREVIEWS in endocrinology\",\"volume\":\"20 2\",\"pages\":\"124-129\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11548356/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"TouchREVIEWS in endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17925/EE.2024.20.2.16\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"TouchREVIEWS in endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17925/EE.2024.20.2.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/2 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
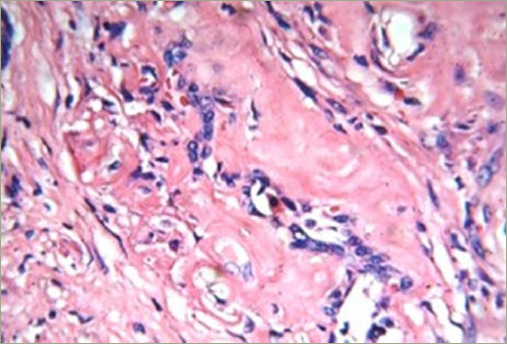
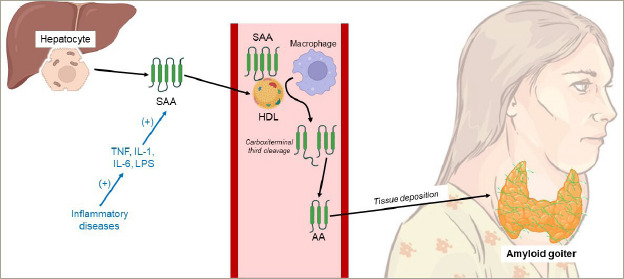
简介淀粉样变性甲状腺肿(AG)是甲状腺肿大的一种罕见病因,其特点是淀粉样蛋白在甲状腺组织中沉积。它可能与原发性或继发性淀粉样变性有关。它在多结节性甲状腺肿病例中的发病率为0.17%,在手术前很少被临床发现。病例系列:这组秘鲁病例包括三名女性患者和一名男性患者,年龄从28岁到65岁不等。所有患者之前都患有炎症性疾病,并报告了呼吸困难、吞咽困难和发音障碍等症状。体格检查显示,所有患者均患有三级甲状腺肿。细针穿刺检查报告为胶状甲状腺肿。四名患者中有三人接受了甲状腺全切除术,组织化学检查显示AG刚果红染色阳性。讨论:AG在临床上并不常见。据报道,它多发于男性,平均诊断年龄为40岁。在我们的系列研究中,我们观察到确诊患者的年龄跨度很大,从 28 岁到 65 岁不等,其中女性居多。对 AG 的考虑应扩展到每一位患有潜在慢性全身性炎症疾病的患者,尤其是终末期肾病患者。在这种情况下,对于多结节性甲状腺肿患者,如我们的系列病例所示,应将AG纳入鉴别诊断,因为AG表现为进行性生长,并在颈椎水平引起压迫症状,但不影响甲状腺功能。结论AG是一种罕见病,在出现巨型甲状腺肿并伴有潜在的全身炎症性疾病时值得怀疑。
Introduction: Amyloid goiter (AG) is a rare cause of thyroid swelling, characterized by deposits of amyloid protein in the thyroid tissue. It can be associated with primary or secondary amyloidosis. Its prevalence in multinodular goiter cases is 0.17%, with rare clinical detection before surgery. Case series: This Peruvian case series comprised three female patients and one male patient, with ages ranging from 28 to 65 years. All individuals had pre-existing inflammatory diseases and reported symptoms including dyspnoea, dysphagia and dysphonia. Upon physical examination, all patients exhibited a grade III goiter. Fine-needle aspiration reported colloid goiter. Three out of the four patients underwent total thyroidectomy and histochemistry revealed AG with positive Congo red staining. Discussion: AG is an uncommon clinical entity. It has been reported to occur more frequently in males, with an average age of diagnosis of 40 years. In our series, we observed a broad age range of patients receiving diagnoses, spanning from 28 to 65 years, with a predominance in females. The consideration of AG should be extended to every patient with an underlying chronic systemic inflammatory disease, especially end stage renal disease. In this context, AG should be included in the differential diagnosis for patients with multinodular goiter exhibiting progressive growth and causing compressive symptoms at the cervical level without affecting thyroid function, as demonstrated in our series. Conclusion: AG, a rare condition, warrants suspicion in the presence of a giant goiter with an underlying systemic inflammatory disease.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
