Kumiko Kirita, Seiji Futagami, Ken Nakamura, Shuhei Agawa, Nobue Ueki, Kazutoshi Higuchi, Mayu Habiro, Rie Kawawa, Yusuke Kato, Tomohiro Tada, Katsuhiko Iwakiri
{"title":"人工智能内镜诊断与内镜专家确定的木村-竹本分级相结合,可有效评估灭活后胃萎缩的分层情况。","authors":"Kumiko Kirita, Seiji Futagami, Ken Nakamura, Shuhei Agawa, Nobue Ueki, Kazutoshi Higuchi, Mayu Habiro, Rie Kawawa, Yusuke Kato, Tomohiro Tada, Katsuhiko Iwakiri","doi":"10.1002/deo2.70029","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Since it is difficult for expert endoscopists to diagnose early gastric cancer in post-eradication status, it may be critical to evaluate the stratification of high-risk groups using the advance of gastric atrophy or intestinal metaplasia. We tried to determine whether the combination of endoscopic artificial intelligence (AI) diagnosis for the evaluation of gastric atrophy could be a useful tool in both pre- and post-eradication status.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>270 <i>Helicobacter pylori</i>-positive outpatients (Study I) were enrolled and Study II was planned to compare patients (<i>n</i> = 72) with pre-eradication therapy with post-eradication therapy. Assessment of endoscopic appearance was evaluated by the Kyoto classification and Kimura-Takemoto classification. The trained neural network generated a continuous number between 0 and 1 for gastric atrophy.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were significant associations between the severity of gastric atrophy determined by AI endoscopic diagnosis and not having a regular arrangement of collecting venules in angle, visibility of vascular pattern, and mucus using Kyoto classification in <i>H. pylori</i>-positive gastritis. There were significant differences (<i>p</i> = 0.037 and <i>p</i> = 0.014) in the severity of gastric atrophy between the high-risk group and low-risk group based on the combination of Kimura-Takemoto classification and endoscopic AI diagnosis in pre- and post-eradication status. The area under the curve values of the severity of gastric atrophy (0.674) determined by the combination of Kimura-Takemoto classification and gastric atrophy determined by AI diagnosis was higher than that determined by Kimura-Takemoto classification alone in post-eradication status.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>A combination of gastric atrophy determined by AI endoscopic diagnosis and Kimura-Takemoto classification may be a useful tool for the prediction of high-risk groups in post-eradication status.</p>\n </section>\n </div>","PeriodicalId":93973,"journal":{"name":"DEN open","volume":"5 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555298/pdf/","citationCount":"0","resultStr":"{\"title\":\"Combination of artificial intelligence endoscopic diagnosis and Kimura-Takemoto classification determined by endoscopic experts may effectively evaluate the stratification of gastric atrophy in post-eradication status\",\"authors\":\"Kumiko Kirita, Seiji Futagami, Ken Nakamura, Shuhei Agawa, Nobue Ueki, Kazutoshi Higuchi, Mayu Habiro, Rie Kawawa, Yusuke Kato, Tomohiro Tada, Katsuhiko Iwakiri\",\"doi\":\"10.1002/deo2.70029\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Since it is difficult for expert endoscopists to diagnose early gastric cancer in post-eradication status, it may be critical to evaluate the stratification of high-risk groups using the advance of gastric atrophy or intestinal metaplasia. We tried to determine whether the combination of endoscopic artificial intelligence (AI) diagnosis for the evaluation of gastric atrophy could be a useful tool in both pre- and post-eradication status.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>270 <i>Helicobacter pylori</i>-positive outpatients (Study I) were enrolled and Study II was planned to compare patients (<i>n</i> = 72) with pre-eradication therapy with post-eradication therapy. Assessment of endoscopic appearance was evaluated by the Kyoto classification and Kimura-Takemoto classification. The trained neural network generated a continuous number between 0 and 1 for gastric atrophy.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>There were significant associations between the severity of gastric atrophy determined by AI endoscopic diagnosis and not having a regular arrangement of collecting venules in angle, visibility of vascular pattern, and mucus using Kyoto classification in <i>H. pylori</i>-positive gastritis. There were significant differences (<i>p</i> = 0.037 and <i>p</i> = 0.014) in the severity of gastric atrophy between the high-risk group and low-risk group based on the combination of Kimura-Takemoto classification and endoscopic AI diagnosis in pre- and post-eradication status. The area under the curve values of the severity of gastric atrophy (0.674) determined by the combination of Kimura-Takemoto classification and gastric atrophy determined by AI diagnosis was higher than that determined by Kimura-Takemoto classification alone in post-eradication status.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>A combination of gastric atrophy determined by AI endoscopic diagnosis and Kimura-Takemoto classification may be a useful tool for the prediction of high-risk groups in post-eradication status.</p>\\n </section>\\n </div>\",\"PeriodicalId\":93973,\"journal\":{\"name\":\"DEN open\",\"volume\":\"5 1\",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-11-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555298/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"DEN open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/deo2.70029\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"DEN open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/deo2.70029","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
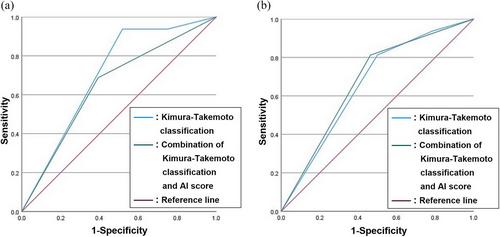
背景:由于内镜专家很难诊断歼灭后状态下的早期胃癌,因此利用胃萎缩或肠化生提前评估高危人群的分层可能至关重要。我们试图确定结合内镜人工智能(AI)诊断来评估胃萎缩是否能成为根治前和根治后状态下的有用工具。方法:270 名幽门螺杆菌阳性门诊患者(研究 I)被纳入研究,研究 II 计划对根治前和根治后患者(n = 72)进行比较。内镜外观评估采用京都分类法和木村-竹本分类法。经过训练的神经网络为胃萎缩生成一个介于 0 和 1 之间的连续数字:结果:在幽门螺杆菌阳性胃炎中,通过 AI 内镜诊断确定的胃萎缩严重程度与角集合静脉排列不规则、血管形态可见度和京都分类法确定的粘液之间存在明显关联。根据木村-竹本分类法和内镜 AI 诊断,在根治前和根治后状态下,高危组和低危组的胃萎缩严重程度存在明显差异(p = 0.037 和 p = 0.014)。根据木村-竹本分类法和内镜 AI 诊断法测定的胃萎缩严重程度的曲线下面积值(0.674)高于单独根据木村-竹本分类法测定的糜烂后胃萎缩严重程度的曲线下面积值:结论:将 AI 内镜诊断确定的胃萎缩与木村-泷本分类相结合,可能是预测根治后高危人群的有效工具。
Combination of artificial intelligence endoscopic diagnosis and Kimura-Takemoto classification determined by endoscopic experts may effectively evaluate the stratification of gastric atrophy in post-eradication status
Background
Since it is difficult for expert endoscopists to diagnose early gastric cancer in post-eradication status, it may be critical to evaluate the stratification of high-risk groups using the advance of gastric atrophy or intestinal metaplasia. We tried to determine whether the combination of endoscopic artificial intelligence (AI) diagnosis for the evaluation of gastric atrophy could be a useful tool in both pre- and post-eradication status.
Methods
270 Helicobacter pylori-positive outpatients (Study I) were enrolled and Study II was planned to compare patients (n = 72) with pre-eradication therapy with post-eradication therapy. Assessment of endoscopic appearance was evaluated by the Kyoto classification and Kimura-Takemoto classification. The trained neural network generated a continuous number between 0 and 1 for gastric atrophy.
Results
There were significant associations between the severity of gastric atrophy determined by AI endoscopic diagnosis and not having a regular arrangement of collecting venules in angle, visibility of vascular pattern, and mucus using Kyoto classification in H. pylori-positive gastritis. There were significant differences (p = 0.037 and p = 0.014) in the severity of gastric atrophy between the high-risk group and low-risk group based on the combination of Kimura-Takemoto classification and endoscopic AI diagnosis in pre- and post-eradication status. The area under the curve values of the severity of gastric atrophy (0.674) determined by the combination of Kimura-Takemoto classification and gastric atrophy determined by AI diagnosis was higher than that determined by Kimura-Takemoto classification alone in post-eradication status.
Conclusion
A combination of gastric atrophy determined by AI endoscopic diagnosis and Kimura-Takemoto classification may be a useful tool for the prediction of high-risk groups in post-eradication status.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
