Hiroki A. Ueyama MD , Kevin F. Kennedy MS , Jennifer A. Rymer MD, MBA, MHS , Alexander T. Sandhu MD, MS , Toshiki Kuno MD, PhD , Frederick A. Masoudi MD, MSPH , John A. Spertus MD, MPH , Shun Kohsaka MD
{"title":"非 ST 段抬高型急性冠状动脉综合征的 P2Y12 抑制剂预处理:NCDR胸痛-MI登记处","authors":"Hiroki A. Ueyama MD , Kevin F. Kennedy MS , Jennifer A. Rymer MD, MBA, MHS , Alexander T. Sandhu MD, MS , Toshiki Kuno MD, PhD , Frederick A. Masoudi MD, MSPH , John A. Spertus MD, MPH , Shun Kohsaka MD","doi":"10.1016/j.jacc.2024.09.1227","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Although high rates of P2Y<sub>12</sub> inhibitor pretreatment (defined as the administration before coronary angiography) for non–ST-segment elevation acute coronary syndrome (NSTE-ACS) have been reported, contemporary U.S. practice patterns are not well studied.</div></div><div><h3>Objectives</h3><div>The goal of this study was to investigate the temporal U.S. trends, variability, and clinical outcomes of P2Y<sub>12</sub> inhibitor pretreatment in NSTE-ACS.</div></div><div><h3>Methods</h3><div>Consecutive patients who underwent early invasive strategy for NSTE-ACS (coronary angiography ≤24 hours of arrival) in the National Cardiovascular Data Registry Chest Pain-Myocardial Infarction (MI) Registry were analyzed. A time-trend analysis was conducted on a complete cohort between January 1, 2013, and March 31, 2023. Subsequently, a more recent cohort (January 1, 2019, to March 31, 2023) with a complete set of variables was used to construct hierarchical regression models to quantify the variability in the use of pretreatment among operators and institutions. For this contemporary cohort, instrumental variable analysis, with operator preference as the instrument, was performed to compare the in-hospital outcomes between patients who received pretreatment and those who did not.</div></div><div><h3>Results</h3><div>Use of P2Y<sub>12</sub> inhibitor pretreatment decreased from 24.8% in 2013Q1 to 12.4% in 2023Q1. Among the contemporary cohort of 110,148 patients (2019-2023; mean age 63.9 ± 12.5 years; 33.0% female), 17,509 (15.9%) received pretreatment. Significant variability in P2Y<sub>12</sub> inhibitor pretreatment was observed (range: 0%-100%): hierarchical regression model demonstrated that 2 similar patients would have a >3-fold difference in the odds of pretreatment from 1 random operator or institution as compared with another (median OR: 3.74 [95% CI: 3.57-3.91] and 3.63 [95% CI: 3.51-3.74], respectively). Instrumental variable analysis demonstrated no significant differences in in-hospital all-cause death (1.5% vs 1.7%; <em>P</em> = 0.07), recurrent MI (0.6% vs 0.6%; <em>P</em> = 0.98), or major bleeding (2.7% vs 2.8%; <em>P</em> = 0.98) with pretreatment. However, in patients who underwent coronary artery bypass surgery, pretreatment was associated with a longer length of stay (11.2 ± 5.1 days vs 9.8 ± 5.0 days; <em>P</em> < 0.01).</div></div><div><h3>Conclusions</h3><div>In a national U.S. registry, we observed significant variability in the use of P2Y<sub>12</sub> inhibitor pretreatment among NSTE-ACS patients. Given the lack of clear advantages and the potential for prolonged hospital stays, our findings highlight the importance of efforts to improve standardization.</div></div>","PeriodicalId":17187,"journal":{"name":"Journal of the American College of Cardiology","volume":"85 4","pages":"Pages 322-334"},"PeriodicalIF":22.3000,"publicationDate":"2025-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"P2Y12 Inhibitor Pretreatment in Non–ST-Segment Elevation Acute Coronary Syndrome\",\"authors\":\"Hiroki A. Ueyama MD , Kevin F. Kennedy MS , Jennifer A. Rymer MD, MBA, MHS , Alexander T. Sandhu MD, MS , Toshiki Kuno MD, PhD , Frederick A. Masoudi MD, MSPH , John A. Spertus MD, MPH , Shun Kohsaka MD\",\"doi\":\"10.1016/j.jacc.2024.09.1227\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><div>Although high rates of P2Y<sub>12</sub> inhibitor pretreatment (defined as the administration before coronary angiography) for non–ST-segment elevation acute coronary syndrome (NSTE-ACS) have been reported, contemporary U.S. practice patterns are not well studied.</div></div><div><h3>Objectives</h3><div>The goal of this study was to investigate the temporal U.S. trends, variability, and clinical outcomes of P2Y<sub>12</sub> inhibitor pretreatment in NSTE-ACS.</div></div><div><h3>Methods</h3><div>Consecutive patients who underwent early invasive strategy for NSTE-ACS (coronary angiography ≤24 hours of arrival) in the National Cardiovascular Data Registry Chest Pain-Myocardial Infarction (MI) Registry were analyzed. A time-trend analysis was conducted on a complete cohort between January 1, 2013, and March 31, 2023. Subsequently, a more recent cohort (January 1, 2019, to March 31, 2023) with a complete set of variables was used to construct hierarchical regression models to quantify the variability in the use of pretreatment among operators and institutions. For this contemporary cohort, instrumental variable analysis, with operator preference as the instrument, was performed to compare the in-hospital outcomes between patients who received pretreatment and those who did not.</div></div><div><h3>Results</h3><div>Use of P2Y<sub>12</sub> inhibitor pretreatment decreased from 24.8% in 2013Q1 to 12.4% in 2023Q1. Among the contemporary cohort of 110,148 patients (2019-2023; mean age 63.9 ± 12.5 years; 33.0% female), 17,509 (15.9%) received pretreatment. Significant variability in P2Y<sub>12</sub> inhibitor pretreatment was observed (range: 0%-100%): hierarchical regression model demonstrated that 2 similar patients would have a >3-fold difference in the odds of pretreatment from 1 random operator or institution as compared with another (median OR: 3.74 [95% CI: 3.57-3.91] and 3.63 [95% CI: 3.51-3.74], respectively). Instrumental variable analysis demonstrated no significant differences in in-hospital all-cause death (1.5% vs 1.7%; <em>P</em> = 0.07), recurrent MI (0.6% vs 0.6%; <em>P</em> = 0.98), or major bleeding (2.7% vs 2.8%; <em>P</em> = 0.98) with pretreatment. However, in patients who underwent coronary artery bypass surgery, pretreatment was associated with a longer length of stay (11.2 ± 5.1 days vs 9.8 ± 5.0 days; <em>P</em> < 0.01).</div></div><div><h3>Conclusions</h3><div>In a national U.S. registry, we observed significant variability in the use of P2Y<sub>12</sub> inhibitor pretreatment among NSTE-ACS patients. Given the lack of clear advantages and the potential for prolonged hospital stays, our findings highlight the importance of efforts to improve standardization.</div></div>\",\"PeriodicalId\":17187,\"journal\":{\"name\":\"Journal of the American College of Cardiology\",\"volume\":\"85 4\",\"pages\":\"Pages 322-334\"},\"PeriodicalIF\":22.3000,\"publicationDate\":\"2025-02-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American College of Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0735109724098437\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Cardiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0735109724098437","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
P2Y12 Inhibitor Pretreatment in Non–ST-Segment Elevation Acute Coronary Syndrome
Background
Although high rates of P2Y12 inhibitor pretreatment (defined as the administration before coronary angiography) for non–ST-segment elevation acute coronary syndrome (NSTE-ACS) have been reported, contemporary U.S. practice patterns are not well studied.
Objectives
The goal of this study was to investigate the temporal U.S. trends, variability, and clinical outcomes of P2Y12 inhibitor pretreatment in NSTE-ACS.
Methods
Consecutive patients who underwent early invasive strategy for NSTE-ACS (coronary angiography ≤24 hours of arrival) in the National Cardiovascular Data Registry Chest Pain-Myocardial Infarction (MI) Registry were analyzed. A time-trend analysis was conducted on a complete cohort between January 1, 2013, and March 31, 2023. Subsequently, a more recent cohort (January 1, 2019, to March 31, 2023) with a complete set of variables was used to construct hierarchical regression models to quantify the variability in the use of pretreatment among operators and institutions. For this contemporary cohort, instrumental variable analysis, with operator preference as the instrument, was performed to compare the in-hospital outcomes between patients who received pretreatment and those who did not.
Results
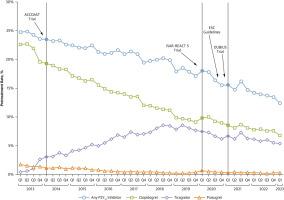
Use of P2Y12 inhibitor pretreatment decreased from 24.8% in 2013Q1 to 12.4% in 2023Q1. Among the contemporary cohort of 110,148 patients (2019-2023; mean age 63.9 ± 12.5 years; 33.0% female), 17,509 (15.9%) received pretreatment. Significant variability in P2Y12 inhibitor pretreatment was observed (range: 0%-100%): hierarchical regression model demonstrated that 2 similar patients would have a >3-fold difference in the odds of pretreatment from 1 random operator or institution as compared with another (median OR: 3.74 [95% CI: 3.57-3.91] and 3.63 [95% CI: 3.51-3.74], respectively). Instrumental variable analysis demonstrated no significant differences in in-hospital all-cause death (1.5% vs 1.7%; P = 0.07), recurrent MI (0.6% vs 0.6%; P = 0.98), or major bleeding (2.7% vs 2.8%; P = 0.98) with pretreatment. However, in patients who underwent coronary artery bypass surgery, pretreatment was associated with a longer length of stay (11.2 ± 5.1 days vs 9.8 ± 5.0 days; P < 0.01).
Conclusions
In a national U.S. registry, we observed significant variability in the use of P2Y12 inhibitor pretreatment among NSTE-ACS patients. Given the lack of clear advantages and the potential for prolonged hospital stays, our findings highlight the importance of efforts to improve standardization.
期刊介绍:
The Journal of the American College of Cardiology (JACC) publishes peer-reviewed articles highlighting all aspects of cardiovascular disease, including original clinical studies, experimental investigations with clear clinical relevance, state-of-the-art papers and viewpoints.
Content Profile:
-Original Investigations
-JACC State-of-the-Art Reviews
-JACC Review Topics of the Week
-Guidelines & Clinical Documents
-JACC Guideline Comparisons
-JACC Scientific Expert Panels
-Cardiovascular Medicine & Society
-Editorial Comments (accompanying every Original Investigation)
-Research Letters
-Fellows-in-Training/Early Career Professional Pages
-Editor’s Pages from the Editor-in-Chief or other invited thought leaders



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
