Marleen A Slim, Rombout B E van Amstel, Marcella C A Müller, Olaf L Cremer, Alexander P J Vlaar, Tom van der Poll, W Joost Wiersinga, Christopher W Seymour, Lonneke A van Vught
{"title":"入住重症监护室的败血症患者的临床亚型轨迹:一项观察性研究的二次分析。","authors":"Marleen A Slim, Rombout B E van Amstel, Marcella C A Müller, Olaf L Cremer, Alexander P J Vlaar, Tom van der Poll, W Joost Wiersinga, Christopher W Seymour, Lonneke A van Vught","doi":"10.1097/CCE.0000000000001176","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Sepsis is an evolving process and proposed subtypes may change over time. We hypothesized that previously established sepsis subtypes are dynamic, prognostic of outcome, and trajectories are associated with host response alterations.</p><p><strong>Design: </strong>A secondary analysis of two observational critically ill sepsis cohorts: the Molecular diAgnosis and Risk stratification of Sepsis (MARS) and the Medical Information Mart for Intensive Care-IV (MIMIC-IV).</p><p><strong>Setting: </strong>ICUs in the Netherlands and United States between 2011-2014 and 2008-2019, respectively.</p><p><strong>Participants: </strong>Patient admission fulfilling the Sepsis-3 criteria upon ICU admission adjudicated to one of four previously identified subtypes, comprising 2,416 admissions in MARS and 10,745 in MIMIC-IV.</p><p><strong>Main outcomes and measures: </strong>Subtype stability and the changes per subtype on days 2, 4 and 7 of ICU admission were assessed. Next, the associated between change in clinical subtype and outcome and host response alterations.</p><p><strong>Results: </strong>In MARS, upon ICU admission, 6% (<i>n</i> = 150) of the patient admissions were α-type, 3% (<i>n</i> = 70) β-type, 55% (<i>n</i> = 1317) γ-type, and 36% (<i>n</i> = 879) δ-type; in MIMIC-IV, this was α = 22% (<i>n</i> = 2398), β = 22% (<i>n</i> = 2365), γ = 31% (<i>n</i> = 3296), and δ = 25% (2686). Overall, prevalence of subtypes was stable over days 2, 4, and 7. However, 28-56% (MARS/MIMIC-IV) changed from α on ICU admission to any of the other subtypes on day 2, 33-71% from β, 57-32% from γ, and 50-48% from δ. On day 4, overall subtype persistence was 33-36%. γ or δ admissions remaining in, or transitioning to, subtype γ on days 2, 4, and 7 exhibited lower mortality rates compared with those remaining in, or transitioning to, subtype δ. Longitudinal host response biomarkers reflecting inflammation, coagulation, and endothelial dysfunction were most altered in the δ-δ group, followed by the γ-δ group, independent of the day or biomarker domain.</p><p><strong>Conclusions and relevance: </strong>In two large cohorts, subtype change to δ was associated with worse clinical outcome and more aberrant biomarkers reflecting inflammation, coagulation, and endothelial dysfunction. These findings underscore the importance of monitoring sepsis subtypes and their linked host responses for improved prognostication and personalized treatment strategies.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 11","pages":"e1176"},"PeriodicalIF":2.9000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11567702/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Subtype Trajectories in Sepsis Patients Admitted to the ICU: A Secondary Analysis of an Observational Study.\",\"authors\":\"Marleen A Slim, Rombout B E van Amstel, Marcella C A Müller, Olaf L Cremer, Alexander P J Vlaar, Tom van der Poll, W Joost Wiersinga, Christopher W Seymour, Lonneke A van Vught\",\"doi\":\"10.1097/CCE.0000000000001176\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Sepsis is an evolving process and proposed subtypes may change over time. We hypothesized that previously established sepsis subtypes are dynamic, prognostic of outcome, and trajectories are associated with host response alterations.</p><p><strong>Design: </strong>A secondary analysis of two observational critically ill sepsis cohorts: the Molecular diAgnosis and Risk stratification of Sepsis (MARS) and the Medical Information Mart for Intensive Care-IV (MIMIC-IV).</p><p><strong>Setting: </strong>ICUs in the Netherlands and United States between 2011-2014 and 2008-2019, respectively.</p><p><strong>Participants: </strong>Patient admission fulfilling the Sepsis-3 criteria upon ICU admission adjudicated to one of four previously identified subtypes, comprising 2,416 admissions in MARS and 10,745 in MIMIC-IV.</p><p><strong>Main outcomes and measures: </strong>Subtype stability and the changes per subtype on days 2, 4 and 7 of ICU admission were assessed. Next, the associated between change in clinical subtype and outcome and host response alterations.</p><p><strong>Results: </strong>In MARS, upon ICU admission, 6% (<i>n</i> = 150) of the patient admissions were α-type, 3% (<i>n</i> = 70) β-type, 55% (<i>n</i> = 1317) γ-type, and 36% (<i>n</i> = 879) δ-type; in MIMIC-IV, this was α = 22% (<i>n</i> = 2398), β = 22% (<i>n</i> = 2365), γ = 31% (<i>n</i> = 3296), and δ = 25% (2686). Overall, prevalence of subtypes was stable over days 2, 4, and 7. However, 28-56% (MARS/MIMIC-IV) changed from α on ICU admission to any of the other subtypes on day 2, 33-71% from β, 57-32% from γ, and 50-48% from δ. On day 4, overall subtype persistence was 33-36%. γ or δ admissions remaining in, or transitioning to, subtype γ on days 2, 4, and 7 exhibited lower mortality rates compared with those remaining in, or transitioning to, subtype δ. Longitudinal host response biomarkers reflecting inflammation, coagulation, and endothelial dysfunction were most altered in the δ-δ group, followed by the γ-δ group, independent of the day or biomarker domain.</p><p><strong>Conclusions and relevance: </strong>In two large cohorts, subtype change to δ was associated with worse clinical outcome and more aberrant biomarkers reflecting inflammation, coagulation, and endothelial dysfunction. These findings underscore the importance of monitoring sepsis subtypes and their linked host responses for improved prognostication and personalized treatment strategies.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"6 11\",\"pages\":\"e1176\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11567702/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001176\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Clinical Subtype Trajectories in Sepsis Patients Admitted to the ICU: A Secondary Analysis of an Observational Study.
Objectives: Sepsis is an evolving process and proposed subtypes may change over time. We hypothesized that previously established sepsis subtypes are dynamic, prognostic of outcome, and trajectories are associated with host response alterations.
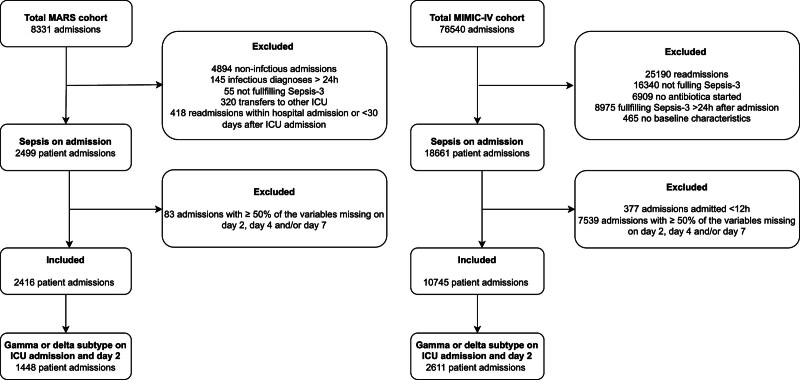
Design: A secondary analysis of two observational critically ill sepsis cohorts: the Molecular diAgnosis and Risk stratification of Sepsis (MARS) and the Medical Information Mart for Intensive Care-IV (MIMIC-IV).
Setting: ICUs in the Netherlands and United States between 2011-2014 and 2008-2019, respectively.
Participants: Patient admission fulfilling the Sepsis-3 criteria upon ICU admission adjudicated to one of four previously identified subtypes, comprising 2,416 admissions in MARS and 10,745 in MIMIC-IV.
Main outcomes and measures: Subtype stability and the changes per subtype on days 2, 4 and 7 of ICU admission were assessed. Next, the associated between change in clinical subtype and outcome and host response alterations.
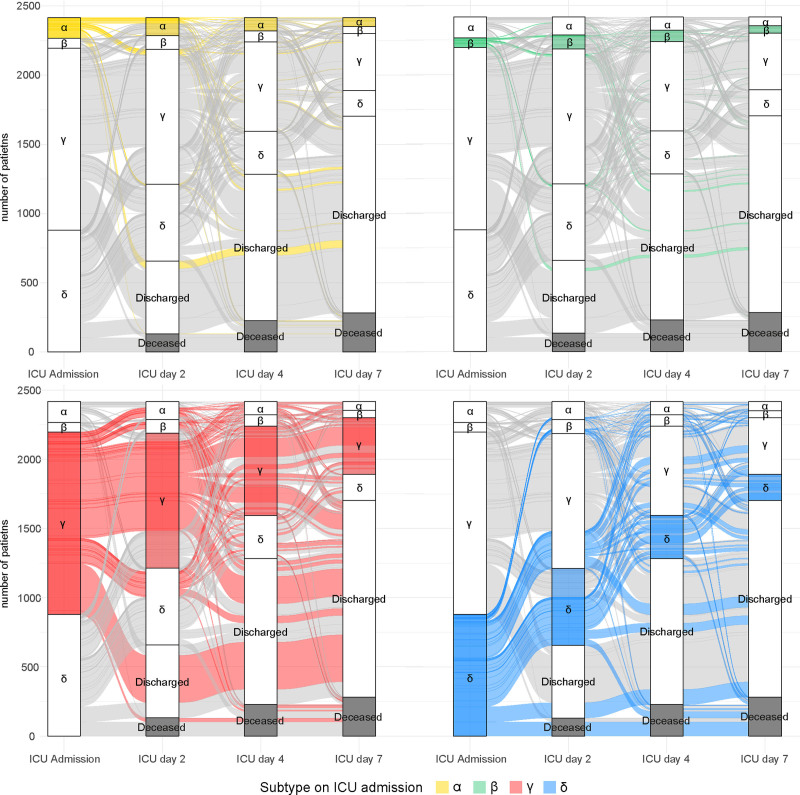
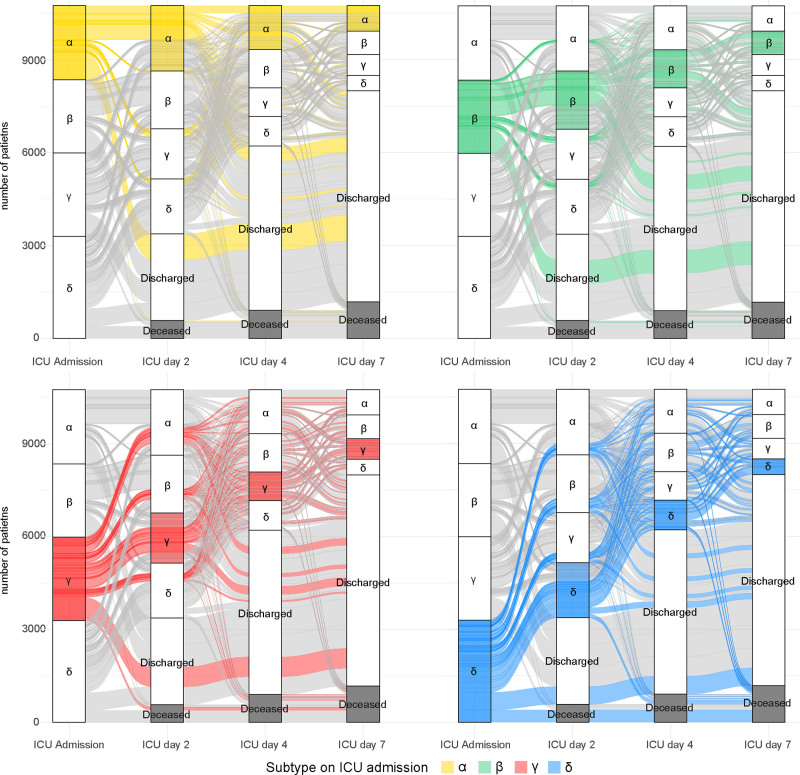
Results: In MARS, upon ICU admission, 6% (n = 150) of the patient admissions were α-type, 3% (n = 70) β-type, 55% (n = 1317) γ-type, and 36% (n = 879) δ-type; in MIMIC-IV, this was α = 22% (n = 2398), β = 22% (n = 2365), γ = 31% (n = 3296), and δ = 25% (2686). Overall, prevalence of subtypes was stable over days 2, 4, and 7. However, 28-56% (MARS/MIMIC-IV) changed from α on ICU admission to any of the other subtypes on day 2, 33-71% from β, 57-32% from γ, and 50-48% from δ. On day 4, overall subtype persistence was 33-36%. γ or δ admissions remaining in, or transitioning to, subtype γ on days 2, 4, and 7 exhibited lower mortality rates compared with those remaining in, or transitioning to, subtype δ. Longitudinal host response biomarkers reflecting inflammation, coagulation, and endothelial dysfunction were most altered in the δ-δ group, followed by the γ-δ group, independent of the day or biomarker domain.
Conclusions and relevance: In two large cohorts, subtype change to δ was associated with worse clinical outcome and more aberrant biomarkers reflecting inflammation, coagulation, and endothelial dysfunction. These findings underscore the importance of monitoring sepsis subtypes and their linked host responses for improved prognostication and personalized treatment strategies.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
