{"title":"依库珠单抗与利妥昔单抗治疗难治性抗乙酰胆碱受体抗体阳性的全身性肌无力:单中心经验","authors":"Hacer Durmus, Arman Çakar, Yesim Gülşen Parman","doi":"10.1155/2024/9924598","DOIUrl":null,"url":null,"abstract":"<p><b>Background:</b> Rituximab (RTX) and eculizumab (ECU) are treatment options for refractory myasthenia gravis (MG), but comparative clinical data derived from real-world experience are limited. Here, we describe the baseline characteristics, treatment, and safety outcomes of patients with antiacetylcholine receptor antibody-positive (AChR+) generalized myasthenia gravis (gMG) treated with ECU and/or RTX in our clinic.</p><p><b>Methods:</b> Patients with refractory AChR+ gMG who received ECU or/and RTX treatment for more than 1 year at the Department of Neurology, Istanbul Faculty of Medicine were included in this observational study. After obtaining written patient consent, data were collected retrospectively from medical records.</p><p><b>Results:</b> Twelve patients treated with ECU and 25 patients treated with RTX were included in the analysis. Groups were comparable with regard to demographic and clinical characteristics, including age at onset of MG, disease duration, and history of thymoma. ECU was associated with significantly better outcomes compared with RTX, as measured by decreases in the mean MG activities of daily living score at 1 (<i>p</i> = 0.024), 3 (<i>p</i> < 0.001), 6 (<i>p</i> < 0.001), and 12 (<i>p</i> < 0.001) months of treatment; steroid-sparing effect after 1 year of treatment (decrease in mean [standard deviation] daily prednisolone dose of −21.8 mg [13.5] vs. −6.6 mg [9.4] with RTX; <i>p</i> < 0.001); and need for rescue treatment and number of myasthenic crisis episodes during treatment (<i>p</i> < 0.001). No new safety signals were observed with either treatment.</p><p><b>Conclusion:</b> Our data provide real-world evidence supporting ECU over RTX to treat patients with refractory AChR+ gMG.</p>","PeriodicalId":6939,"journal":{"name":"Acta Neurologica Scandinavica","volume":"2024 1","pages":""},"PeriodicalIF":2.7000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/9924598","citationCount":"0","resultStr":"{\"title\":\"Eculizumab Versus Rituximab for Refractory Antiacetylcholine Receptor Antibody-Positive Generalized Myasthenia Gravis: A Single-Center Experience\",\"authors\":\"Hacer Durmus, Arman Çakar, Yesim Gülşen Parman\",\"doi\":\"10.1155/2024/9924598\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>Background:</b> Rituximab (RTX) and eculizumab (ECU) are treatment options for refractory myasthenia gravis (MG), but comparative clinical data derived from real-world experience are limited. Here, we describe the baseline characteristics, treatment, and safety outcomes of patients with antiacetylcholine receptor antibody-positive (AChR+) generalized myasthenia gravis (gMG) treated with ECU and/or RTX in our clinic.</p><p><b>Methods:</b> Patients with refractory AChR+ gMG who received ECU or/and RTX treatment for more than 1 year at the Department of Neurology, Istanbul Faculty of Medicine were included in this observational study. After obtaining written patient consent, data were collected retrospectively from medical records.</p><p><b>Results:</b> Twelve patients treated with ECU and 25 patients treated with RTX were included in the analysis. Groups were comparable with regard to demographic and clinical characteristics, including age at onset of MG, disease duration, and history of thymoma. ECU was associated with significantly better outcomes compared with RTX, as measured by decreases in the mean MG activities of daily living score at 1 (<i>p</i> = 0.024), 3 (<i>p</i> < 0.001), 6 (<i>p</i> < 0.001), and 12 (<i>p</i> < 0.001) months of treatment; steroid-sparing effect after 1 year of treatment (decrease in mean [standard deviation] daily prednisolone dose of −21.8 mg [13.5] vs. −6.6 mg [9.4] with RTX; <i>p</i> < 0.001); and need for rescue treatment and number of myasthenic crisis episodes during treatment (<i>p</i> < 0.001). No new safety signals were observed with either treatment.</p><p><b>Conclusion:</b> Our data provide real-world evidence supporting ECU over RTX to treat patients with refractory AChR+ gMG.</p>\",\"PeriodicalId\":6939,\"journal\":{\"name\":\"Acta Neurologica Scandinavica\",\"volume\":\"2024 1\",\"pages\":\"\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/9924598\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Neurologica Scandinavica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/2024/9924598\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Neurologica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/9924598","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Eculizumab Versus Rituximab for Refractory Antiacetylcholine Receptor Antibody-Positive Generalized Myasthenia Gravis: A Single-Center Experience
Background: Rituximab (RTX) and eculizumab (ECU) are treatment options for refractory myasthenia gravis (MG), but comparative clinical data derived from real-world experience are limited. Here, we describe the baseline characteristics, treatment, and safety outcomes of patients with antiacetylcholine receptor antibody-positive (AChR+) generalized myasthenia gravis (gMG) treated with ECU and/or RTX in our clinic.
Methods: Patients with refractory AChR+ gMG who received ECU or/and RTX treatment for more than 1 year at the Department of Neurology, Istanbul Faculty of Medicine were included in this observational study. After obtaining written patient consent, data were collected retrospectively from medical records.
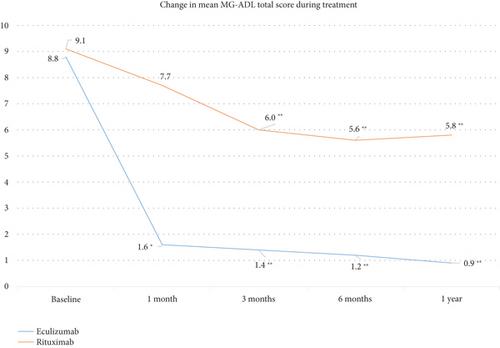
Results: Twelve patients treated with ECU and 25 patients treated with RTX were included in the analysis. Groups were comparable with regard to demographic and clinical characteristics, including age at onset of MG, disease duration, and history of thymoma. ECU was associated with significantly better outcomes compared with RTX, as measured by decreases in the mean MG activities of daily living score at 1 (p = 0.024), 3 (p < 0.001), 6 (p < 0.001), and 12 (p < 0.001) months of treatment; steroid-sparing effect after 1 year of treatment (decrease in mean [standard deviation] daily prednisolone dose of −21.8 mg [13.5] vs. −6.6 mg [9.4] with RTX; p < 0.001); and need for rescue treatment and number of myasthenic crisis episodes during treatment (p < 0.001). No new safety signals were observed with either treatment.
Conclusion: Our data provide real-world evidence supporting ECU over RTX to treat patients with refractory AChR+ gMG.
期刊介绍:
Acta Neurologica Scandinavica aims to publish manuscripts of a high scientific quality representing original clinical, diagnostic or experimental work in neuroscience. The journal''s scope is to act as an international forum for the dissemination of information advancing the science or practice of this subject area. Papers in English will be welcomed, especially those which bring new knowledge and observations from the application of therapies or techniques in the combating of a broad spectrum of neurological disease and neurodegenerative disorders. Relevant articles on the basic neurosciences will be published where they extend present understanding of such disorders. Priority will be given to review of topical subjects. Papers requiring rapid publication because of their significance and timeliness will be included as ''Clinical commentaries'' not exceeding two printed pages, as will ''Clinical commentaries'' of sufficient general interest. Debate within the speciality is encouraged in the form of ''Letters to the editor''. All submitted manuscripts falling within the overall scope of the journal will be assessed by suitably qualified referees.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
