{"title":"以双侧 Parvus et Tardus 肾脏多普勒血流模式为诊断途径,延迟发现老年人主动脉共动脉瘤导致的抵抗性高血压--病例报告。","authors":"Jeevan Ghimire, Prabin Shrestha, Sushan Homagain, Suruchi Paudel, Rabin Bhusal","doi":"10.1002/ccr3.9587","DOIUrl":null,"url":null,"abstract":"<p>Coarctation of the aorta is the narrowing of the aorta distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”) [<span>5</span>]. Coarctation of the aorta is a congenital cardiovascular condition, and it accounts for 5%–10% of all congenital cardiovascular diseases. Coarctation of the aorta can occur at any region in the thoracic and abdominal aorta. The most common location for coarctation of the aorta is just distal to the left subclavian artery at the point where ductus arteriosus connects to the aorta [<span>3</span>]. The majority of coarctation of the aorta cases are commonly diagnosed during childhood; however, many cases remain asymptomatic until adulthood [<span>2</span>]. In the adult population, coarctation of the aorta commonly presents with secondary hypertension (particularly upper extremity hypertension), radio femoral delay with absent or weak palpable femoral pulses, and left ventricular hypertrophy [<span>7</span>]. Here we present a case of delayed detection of coarctation of the aorta as a cause of secondary hypertension in an adult male with absence of typical clinical signs, leading to delay in diagnosis in the rural setting.</p><p>A 48-years-old male, known case of hypertension under medication for 7 years with no other comorbidities, presented with complaints of gradually progressive shortness of breath and headache for 6 months. There was no history of palpitation, orthopnea, paroxysmal nocturnal dyspnea, limb swelling, blurred vision, or focal neurological deficits. He had a smoking history of 10 pack years and was a social drinker. There is no significant family history. The patient was taking four antihypertensive drugs (amlodipine 10 mg OD, prazosin XL 5 mg TDS, clonidine 100 mg BD, hydrochlorothiazide 12.5 mg BD). On examination, he had elevated blood pressure (BP) measured in the sitting position (180/110 mmHg on bilateral arms). There was no edema, cyanosis or digital clubbing. Radio-radial and radio-femoral delay were not present. Systemic examinations were at normal limits. Investigations were ordered to search for the secondary cause of the resistant hypertension as well as evaluate for end organ damage, if any.</p><p>Routine blood investigations were within normal limits, with normal renal function test (RFT), thyroid function test (TFT), urine metanephrines, and normetanephrines as shown in Table 1.</p><p>On radiological investigations, renal Doppler showed parvus et tardus waveform in both main renal arteries and interlobar arteries with reduced velocities and decreased acceleration time suggestive of Renal Artery stenosis (Figure 1). Echocardiography was performed to see the effect caused by hypertension in heart showed abrupt tapering of descending thoracic aorta distal to left subclavian artery with mild concentric left ventricular hypertrophy (LVH) with ejection fraction (EF) 60%, features suggesting anomaly of aorta (Figure 2). Computed tomography(CT) of the chest and the abdomen revealed non-visualized proximal most descending thoracic aorta with narrowed proximal segment in partially included arch of aorta with prominent collaterals in chest wall, bilateral axillary region, abdomen, rectus abdominis, and prominent bilateral inferior epigastric artery (Figures 3 and 4). The radiologist then advised for CT thoracic aortogram with differentials of coarctation of the aorta and interrupted aortic Arch. CT thoracic aortogram showed abrupt interruption of proximal descending thoracic aorta approximately 1.6 cm distal to origin of left subclavian artery features suggestive of coarctation of the aorta with markedly prominent chest wall and anterior abdominal wall collaterals (Figure 5). X-ray of the chest showed notching of ribs (Figure 6).</p><p>The diagnosis of systemic hypertension secondary to post–ductal coarctation of the aorta and bilateral renal artery stenosis was thus established. The patient was planned for coarctation of aorta repair with resection and interposition graft. Per operatively, post–ductal coarctation of descending thoracic aorta 2 cm distal to ligamentum arteriosum with prominent collaterals was noticed. Postoperative chest X-ray is shown in Figure 7.</p><p>The postoperative period was uneventful and the patient was discharged 10 days later. At the time of discharge, blood pressure of the upper limb was 120/70 mmHg in sitting position while that of the lower limb was 130/80 mmHg with palpable peripheral pulse and no radio-femoral delay. The patient was advised for continuation of antihypertensive medication (amlodipine 5 mg OD, prazosin 5 mg OD) and was scheduled for regular follow-up 6 monthly. The patient is doing well in subsequent visits with maintained blood pressure ranges.</p><p>Coarctation of the aorta is the congenital narrowing of the aorta just distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”). It can remain asymptomatic during childhood and present as secondary hypertension and left ventricular hypertrophy during adulthood [<span>2</span>].</p><p>The diagnosis of coarctation of the aorta may go unrecognized if the physician does not think of coarctation of the aorta as a possible secondary cause of hypertension. Coarctation of the aorta is a congenital malformation, which can cause systemic hypertension and subsequent complications. Because hypertension caused by coarctation of the aorta tends to be resistant to medical therapy, early detection and surgical correction are important. Although discrepancies between arm and leg BP and the presence of bruits due to narrowing lesions can aid in the diagnosis of coarctation of the aorta, sometimes these signs are not obvious or can be overlooked [<span>4</span>]. In our case, blood pressure of the lower extremities was not determined, and if it was recorded and discrepancies were present in the reading, the patient would have benefited earlier. Radio-femoral delay is not always present in coarctation of the aorta. While it is a common finding in many cases, it is not a universal characteristic of the condition [<span>8</span>]. Hypertension in such patients may be controlled only after the correction of coarctation of the aorta, with surgical repair or balloon angioplasty with stent placement [<span>7</span>]. Resection with interposition graft replacement provides a safe and durable repair option compared to endovascular stenting [<span>1</span>].</p><p>All of the signs of coarctation of the aorta were absent and it was resistant to multiple antihypertensive drugs thus prompting a search for secondary causes of hypertension. Ultrasonography Doppler (USG Doppler) showed bilateral parvus et tardus waveform with normal renal function test in laboratory investigations. When bilateral tardus-parvus wave patterns are detected, bilateral renal artery stenosis, aortic stenosis, and coarctation of the aorta should be considered [<span>9</span>]. Early detection and prompt treatment of coarctation of the aorta can prevent many complications in patients. Most of the patients with undetected coarctation of the aorta die within 50 years due to cardiovascular complications. The mortality reported in patients with coarctation of the aorta is due to coronary artery disease, heart failure, aortic rupture, endocarditis, cerebrovascular accidents [<span>6</span>].</p><p>This case report shows that clinicians must be mindful about secondary causes when a patient presents with resistant hypertension. Coarctation of the aorta is an important cause of secondary hypertension and may not present with typical signs during clinical examination, so considering it even in the absence of signs can decrease the mortality related to it, which can be treated through surgical intervention. Even in the absence of typical physical signs, renal Doppler with bilateral parvus et tardus flow pattern aids to reconsider coarctation of the aorta as a differential diagnosis and investigate to confirm it. Most of the patients with untreated coarctation die of cardiovascular complications, which can be prevented by early diagnosis and treatment.</p><p><b>Jeevan Ghimire:</b> conceptualization, writing – original draft, writing – review and editing. <b>Prabin Shrestha:</b> writing – original draft. <b>Sushan Homagain:</b> writing – original draft, writing – review and editing. <b>Suruchi Paudel:</b> writing – review and editing. <b>Rabin Bhusal:</b> writing – review and editing.</p><p>Written informed consent was obtained from the parents to publish this report in accordance with the journal's patient consent policy.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":10327,"journal":{"name":"Clinical Case Reports","volume":"12 11","pages":""},"PeriodicalIF":0.6000,"publicationDate":"2024-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11570417/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed Detection of Coarctation of the Aorta Causing Resistant Hypertension in Elderly With Bilateral Parvus et Tardus Renal Doppler Flow Pattern Serving as a Gateway to Diagnosis—A Case Report\",\"authors\":\"Jeevan Ghimire, Prabin Shrestha, Sushan Homagain, Suruchi Paudel, Rabin Bhusal\",\"doi\":\"10.1002/ccr3.9587\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Coarctation of the aorta is the narrowing of the aorta distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”) [<span>5</span>]. Coarctation of the aorta is a congenital cardiovascular condition, and it accounts for 5%–10% of all congenital cardiovascular diseases. Coarctation of the aorta can occur at any region in the thoracic and abdominal aorta. The most common location for coarctation of the aorta is just distal to the left subclavian artery at the point where ductus arteriosus connects to the aorta [<span>3</span>]. The majority of coarctation of the aorta cases are commonly diagnosed during childhood; however, many cases remain asymptomatic until adulthood [<span>2</span>]. In the adult population, coarctation of the aorta commonly presents with secondary hypertension (particularly upper extremity hypertension), radio femoral delay with absent or weak palpable femoral pulses, and left ventricular hypertrophy [<span>7</span>]. Here we present a case of delayed detection of coarctation of the aorta as a cause of secondary hypertension in an adult male with absence of typical clinical signs, leading to delay in diagnosis in the rural setting.</p><p>A 48-years-old male, known case of hypertension under medication for 7 years with no other comorbidities, presented with complaints of gradually progressive shortness of breath and headache for 6 months. There was no history of palpitation, orthopnea, paroxysmal nocturnal dyspnea, limb swelling, blurred vision, or focal neurological deficits. He had a smoking history of 10 pack years and was a social drinker. There is no significant family history. The patient was taking four antihypertensive drugs (amlodipine 10 mg OD, prazosin XL 5 mg TDS, clonidine 100 mg BD, hydrochlorothiazide 12.5 mg BD). On examination, he had elevated blood pressure (BP) measured in the sitting position (180/110 mmHg on bilateral arms). There was no edema, cyanosis or digital clubbing. Radio-radial and radio-femoral delay were not present. Systemic examinations were at normal limits. Investigations were ordered to search for the secondary cause of the resistant hypertension as well as evaluate for end organ damage, if any.</p><p>Routine blood investigations were within normal limits, with normal renal function test (RFT), thyroid function test (TFT), urine metanephrines, and normetanephrines as shown in Table 1.</p><p>On radiological investigations, renal Doppler showed parvus et tardus waveform in both main renal arteries and interlobar arteries with reduced velocities and decreased acceleration time suggestive of Renal Artery stenosis (Figure 1). Echocardiography was performed to see the effect caused by hypertension in heart showed abrupt tapering of descending thoracic aorta distal to left subclavian artery with mild concentric left ventricular hypertrophy (LVH) with ejection fraction (EF) 60%, features suggesting anomaly of aorta (Figure 2). Computed tomography(CT) of the chest and the abdomen revealed non-visualized proximal most descending thoracic aorta with narrowed proximal segment in partially included arch of aorta with prominent collaterals in chest wall, bilateral axillary region, abdomen, rectus abdominis, and prominent bilateral inferior epigastric artery (Figures 3 and 4). The radiologist then advised for CT thoracic aortogram with differentials of coarctation of the aorta and interrupted aortic Arch. CT thoracic aortogram showed abrupt interruption of proximal descending thoracic aorta approximately 1.6 cm distal to origin of left subclavian artery features suggestive of coarctation of the aorta with markedly prominent chest wall and anterior abdominal wall collaterals (Figure 5). X-ray of the chest showed notching of ribs (Figure 6).</p><p>The diagnosis of systemic hypertension secondary to post–ductal coarctation of the aorta and bilateral renal artery stenosis was thus established. The patient was planned for coarctation of aorta repair with resection and interposition graft. Per operatively, post–ductal coarctation of descending thoracic aorta 2 cm distal to ligamentum arteriosum with prominent collaterals was noticed. Postoperative chest X-ray is shown in Figure 7.</p><p>The postoperative period was uneventful and the patient was discharged 10 days later. At the time of discharge, blood pressure of the upper limb was 120/70 mmHg in sitting position while that of the lower limb was 130/80 mmHg with palpable peripheral pulse and no radio-femoral delay. The patient was advised for continuation of antihypertensive medication (amlodipine 5 mg OD, prazosin 5 mg OD) and was scheduled for regular follow-up 6 monthly. The patient is doing well in subsequent visits with maintained blood pressure ranges.</p><p>Coarctation of the aorta is the congenital narrowing of the aorta just distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”). It can remain asymptomatic during childhood and present as secondary hypertension and left ventricular hypertrophy during adulthood [<span>2</span>].</p><p>The diagnosis of coarctation of the aorta may go unrecognized if the physician does not think of coarctation of the aorta as a possible secondary cause of hypertension. Coarctation of the aorta is a congenital malformation, which can cause systemic hypertension and subsequent complications. Because hypertension caused by coarctation of the aorta tends to be resistant to medical therapy, early detection and surgical correction are important. Although discrepancies between arm and leg BP and the presence of bruits due to narrowing lesions can aid in the diagnosis of coarctation of the aorta, sometimes these signs are not obvious or can be overlooked [<span>4</span>]. In our case, blood pressure of the lower extremities was not determined, and if it was recorded and discrepancies were present in the reading, the patient would have benefited earlier. Radio-femoral delay is not always present in coarctation of the aorta. While it is a common finding in many cases, it is not a universal characteristic of the condition [<span>8</span>]. Hypertension in such patients may be controlled only after the correction of coarctation of the aorta, with surgical repair or balloon angioplasty with stent placement [<span>7</span>]. Resection with interposition graft replacement provides a safe and durable repair option compared to endovascular stenting [<span>1</span>].</p><p>All of the signs of coarctation of the aorta were absent and it was resistant to multiple antihypertensive drugs thus prompting a search for secondary causes of hypertension. Ultrasonography Doppler (USG Doppler) showed bilateral parvus et tardus waveform with normal renal function test in laboratory investigations. When bilateral tardus-parvus wave patterns are detected, bilateral renal artery stenosis, aortic stenosis, and coarctation of the aorta should be considered [<span>9</span>]. Early detection and prompt treatment of coarctation of the aorta can prevent many complications in patients. Most of the patients with undetected coarctation of the aorta die within 50 years due to cardiovascular complications. The mortality reported in patients with coarctation of the aorta is due to coronary artery disease, heart failure, aortic rupture, endocarditis, cerebrovascular accidents [<span>6</span>].</p><p>This case report shows that clinicians must be mindful about secondary causes when a patient presents with resistant hypertension. Coarctation of the aorta is an important cause of secondary hypertension and may not present with typical signs during clinical examination, so considering it even in the absence of signs can decrease the mortality related to it, which can be treated through surgical intervention. Even in the absence of typical physical signs, renal Doppler with bilateral parvus et tardus flow pattern aids to reconsider coarctation of the aorta as a differential diagnosis and investigate to confirm it. Most of the patients with untreated coarctation die of cardiovascular complications, which can be prevented by early diagnosis and treatment.</p><p><b>Jeevan Ghimire:</b> conceptualization, writing – original draft, writing – review and editing. <b>Prabin Shrestha:</b> writing – original draft. <b>Sushan Homagain:</b> writing – original draft, writing – review and editing. <b>Suruchi Paudel:</b> writing – review and editing. <b>Rabin Bhusal:</b> writing – review and editing.</p><p>Written informed consent was obtained from the parents to publish this report in accordance with the journal's patient consent policy.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":10327,\"journal\":{\"name\":\"Clinical Case Reports\",\"volume\":\"12 11\",\"pages\":\"\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-11-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11570417/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ccr3.9587\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccr3.9587","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Delayed Detection of Coarctation of the Aorta Causing Resistant Hypertension in Elderly With Bilateral Parvus et Tardus Renal Doppler Flow Pattern Serving as a Gateway to Diagnosis—A Case Report
Coarctation of the aorta is the narrowing of the aorta distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”) [5]. Coarctation of the aorta is a congenital cardiovascular condition, and it accounts for 5%–10% of all congenital cardiovascular diseases. Coarctation of the aorta can occur at any region in the thoracic and abdominal aorta. The most common location for coarctation of the aorta is just distal to the left subclavian artery at the point where ductus arteriosus connects to the aorta [3]. The majority of coarctation of the aorta cases are commonly diagnosed during childhood; however, many cases remain asymptomatic until adulthood [2]. In the adult population, coarctation of the aorta commonly presents with secondary hypertension (particularly upper extremity hypertension), radio femoral delay with absent or weak palpable femoral pulses, and left ventricular hypertrophy [7]. Here we present a case of delayed detection of coarctation of the aorta as a cause of secondary hypertension in an adult male with absence of typical clinical signs, leading to delay in diagnosis in the rural setting.
A 48-years-old male, known case of hypertension under medication for 7 years with no other comorbidities, presented with complaints of gradually progressive shortness of breath and headache for 6 months. There was no history of palpitation, orthopnea, paroxysmal nocturnal dyspnea, limb swelling, blurred vision, or focal neurological deficits. He had a smoking history of 10 pack years and was a social drinker. There is no significant family history. The patient was taking four antihypertensive drugs (amlodipine 10 mg OD, prazosin XL 5 mg TDS, clonidine 100 mg BD, hydrochlorothiazide 12.5 mg BD). On examination, he had elevated blood pressure (BP) measured in the sitting position (180/110 mmHg on bilateral arms). There was no edema, cyanosis or digital clubbing. Radio-radial and radio-femoral delay were not present. Systemic examinations were at normal limits. Investigations were ordered to search for the secondary cause of the resistant hypertension as well as evaluate for end organ damage, if any.
Routine blood investigations were within normal limits, with normal renal function test (RFT), thyroid function test (TFT), urine metanephrines, and normetanephrines as shown in Table 1.
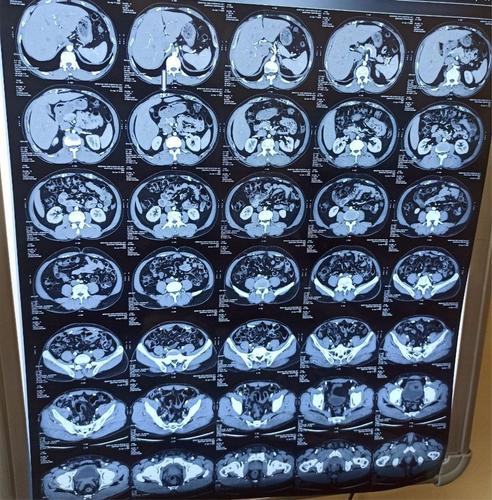
On radiological investigations, renal Doppler showed parvus et tardus waveform in both main renal arteries and interlobar arteries with reduced velocities and decreased acceleration time suggestive of Renal Artery stenosis (Figure 1). Echocardiography was performed to see the effect caused by hypertension in heart showed abrupt tapering of descending thoracic aorta distal to left subclavian artery with mild concentric left ventricular hypertrophy (LVH) with ejection fraction (EF) 60%, features suggesting anomaly of aorta (Figure 2). Computed tomography(CT) of the chest and the abdomen revealed non-visualized proximal most descending thoracic aorta with narrowed proximal segment in partially included arch of aorta with prominent collaterals in chest wall, bilateral axillary region, abdomen, rectus abdominis, and prominent bilateral inferior epigastric artery (Figures 3 and 4). The radiologist then advised for CT thoracic aortogram with differentials of coarctation of the aorta and interrupted aortic Arch. CT thoracic aortogram showed abrupt interruption of proximal descending thoracic aorta approximately 1.6 cm distal to origin of left subclavian artery features suggestive of coarctation of the aorta with markedly prominent chest wall and anterior abdominal wall collaterals (Figure 5). X-ray of the chest showed notching of ribs (Figure 6).
The diagnosis of systemic hypertension secondary to post–ductal coarctation of the aorta and bilateral renal artery stenosis was thus established. The patient was planned for coarctation of aorta repair with resection and interposition graft. Per operatively, post–ductal coarctation of descending thoracic aorta 2 cm distal to ligamentum arteriosum with prominent collaterals was noticed. Postoperative chest X-ray is shown in Figure 7.
The postoperative period was uneventful and the patient was discharged 10 days later. At the time of discharge, blood pressure of the upper limb was 120/70 mmHg in sitting position while that of the lower limb was 130/80 mmHg with palpable peripheral pulse and no radio-femoral delay. The patient was advised for continuation of antihypertensive medication (amlodipine 5 mg OD, prazosin 5 mg OD) and was scheduled for regular follow-up 6 monthly. The patient is doing well in subsequent visits with maintained blood pressure ranges.
Coarctation of the aorta is the congenital narrowing of the aorta just distal to the left subclavian artery near the insertion/opening of ductus arteriosus (i.e., “juxta ductal”). It can remain asymptomatic during childhood and present as secondary hypertension and left ventricular hypertrophy during adulthood [2].
The diagnosis of coarctation of the aorta may go unrecognized if the physician does not think of coarctation of the aorta as a possible secondary cause of hypertension. Coarctation of the aorta is a congenital malformation, which can cause systemic hypertension and subsequent complications. Because hypertension caused by coarctation of the aorta tends to be resistant to medical therapy, early detection and surgical correction are important. Although discrepancies between arm and leg BP and the presence of bruits due to narrowing lesions can aid in the diagnosis of coarctation of the aorta, sometimes these signs are not obvious or can be overlooked [4]. In our case, blood pressure of the lower extremities was not determined, and if it was recorded and discrepancies were present in the reading, the patient would have benefited earlier. Radio-femoral delay is not always present in coarctation of the aorta. While it is a common finding in many cases, it is not a universal characteristic of the condition [8]. Hypertension in such patients may be controlled only after the correction of coarctation of the aorta, with surgical repair or balloon angioplasty with stent placement [7]. Resection with interposition graft replacement provides a safe and durable repair option compared to endovascular stenting [1].
All of the signs of coarctation of the aorta were absent and it was resistant to multiple antihypertensive drugs thus prompting a search for secondary causes of hypertension. Ultrasonography Doppler (USG Doppler) showed bilateral parvus et tardus waveform with normal renal function test in laboratory investigations. When bilateral tardus-parvus wave patterns are detected, bilateral renal artery stenosis, aortic stenosis, and coarctation of the aorta should be considered [9]. Early detection and prompt treatment of coarctation of the aorta can prevent many complications in patients. Most of the patients with undetected coarctation of the aorta die within 50 years due to cardiovascular complications. The mortality reported in patients with coarctation of the aorta is due to coronary artery disease, heart failure, aortic rupture, endocarditis, cerebrovascular accidents [6].
This case report shows that clinicians must be mindful about secondary causes when a patient presents with resistant hypertension. Coarctation of the aorta is an important cause of secondary hypertension and may not present with typical signs during clinical examination, so considering it even in the absence of signs can decrease the mortality related to it, which can be treated through surgical intervention. Even in the absence of typical physical signs, renal Doppler with bilateral parvus et tardus flow pattern aids to reconsider coarctation of the aorta as a differential diagnosis and investigate to confirm it. Most of the patients with untreated coarctation die of cardiovascular complications, which can be prevented by early diagnosis and treatment.
Jeevan Ghimire: conceptualization, writing – original draft, writing – review and editing. Prabin Shrestha: writing – original draft. Sushan Homagain: writing – original draft, writing – review and editing. Suruchi Paudel: writing – review and editing. Rabin Bhusal: writing – review and editing.
Written informed consent was obtained from the parents to publish this report in accordance with the journal's patient consent policy.
期刊介绍:
Clinical Case Reports is different from other case report journals. Our aim is to directly improve global health and increase clinical understanding using case reports to convey important best practice information. We welcome case reports from all areas of Medicine, Nursing, Dentistry, and Veterinary Science and may include: -Any clinical case or procedure which illustrates an important best practice teaching message -Any clinical case or procedure which illustrates the appropriate use of an important clinical guideline or systematic review. As well as: -The management of novel or very uncommon diseases -A common disease presenting in an uncommon way -An uncommon disease masquerading as something more common -Cases which expand understanding of disease pathogenesis -Cases where the teaching point is based on an error -Cases which allow us to re-think established medical lore -Unreported adverse effects of interventions (drug, procedural, or other).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
