{"title":"经支气管冷冻活组织检查诊断培养阴性纤毛膜结核病","authors":"Atif Saleem Siddiqui","doi":"10.1002/ccr3.9595","DOIUrl":null,"url":null,"abstract":"<p>A 19-year-old male with no known medical comorbidities presented to the emergency department with a dry cough and shortness of breath for 3 months. His heart rate was 114/min, respiratory rate was 32/min, blood pressure was 110/80 mmHg, temperature was 101.5 °F, and oxygen saturation was 86% on room air. Initial laboratory data were normal, and a serum Quantiferon test was positive. Computed tomography (CT) of the chest showed bilateral diffuse miliary infiltrates and ground-glass opacities (GGO), with mild bronchiectasis in the left upper lobe (Figure 1A). He required heated high-flow oxygen in the emergency department; however, he was intubated due to worsening respiratory failure and increased work of breathing. Bronchoscopy with bronchoalveolar lavage (BAL) was performed. BAL and tracheal aspirates were negative for <i>Mycobacterium tuberculosis</i> (MTB) polymerase chain reaction (PCR), acid-fast bacilli (AFB), bacterial, and fungal cultures. He remained on mechanical ventilation for 1 week, and all his cultures were negative. A second bronchoscopy with transbronchial cryobiopsy (TBLC) was performed to obtain a tissue diagnosis. TBLC revealed caseating granulomas and multinucleated giant cells (Figure 1B). Grocott's methenamine silver stain was negative. Tissue AFB cultures and MTB PCR obtained via TBLC came back positive for tuberculosis within 1 week. The patient was started on rifampin, isoniazid, pyrazinamide, and ethambutol for a 6-month course. He required a tracheostomy 16 days after mechanical ventilation and was able to wean off mechanical ventilation, being successfully decannulated 2 weeks after the tracheostomy.</p><p>Miliary tuberculosis is a life-threatening hematogenous dissemination of <i>Mycobacterium tuberculosis</i> bacilli. The diagnosis of pulmonary tuberculosis is determined by symptoms, risk factors, sputum smear microscopy, and chest radiography. In miliary TB, acid-fast bacilli (AFB) smears are positive in only 20%–25% of cases, and cultures of sputum are positive in 30%–65% of patients [<span>1</span>]. Transbronchial biopsy diagnostic yields are 62.5%–76% [<span>2</span>]. TBLC has been widely used for the diagnosis of interstitial lung disease. However, the role of TBLC in the diagnosis of culture-negative miliary TB remains unclear. There is limited data on the use of TBLC in culture-negative miliary TB. A case report by Nasu et al. [<span>3</span>] demonstrated the utility of TBLC in diagnosing miliary tuberculosis that initially mimicked hypersensitivity pneumonitis. In this case, cryobiopsy specimens revealed necrotic granulomas, which led to a re-examination of sputum and subsequent identification of <i>Mycobacterium tuberculosis</i>. The patient described in our case had ground-glass opacities (GGO), a rare presentation of miliary TB. Furthermore, sputum and BAL AFB cultures, as well as MTB PCR, were negative. Additionally, Sánchez-Cabral et al. highlighted the diagnostic value of TBLC in non-interstitial lung diseases, including infectious diseases like TB. The study reported a high diagnostic yield when TBLC was combined with bronchoalveolar lavage (BAL), suggesting that TBLC can be a robust diagnostic tool in cases where traditional methods are inconclusive. This case contributes to the limited pool of literature, highlighting the use of TBLC in miliary TB in patients with negative BAL and tracheal aspirates. Furthermore, GGO is an uncommon CT chest characteristic of disseminated TB and can be associated with serious complications. In conclusion, further studies are needed to determine the utility and diagnostic yield of TBLC in this patient population.</p><p><b>Atif Saleem Siddiqui:</b> conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualization, writing – original draft, writing – review and editing.</p><p>Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.</p><p>The author declares no conflicts of interest.</p>","PeriodicalId":10327,"journal":{"name":"Clinical Case Reports","volume":"12 11","pages":""},"PeriodicalIF":0.6000,"publicationDate":"2024-11-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccr3.9595","citationCount":"0","resultStr":"{\"title\":\"Transbronchial Cryobiopsy for the Diagnosis of Culture Negative Miliary Tuberculosis\",\"authors\":\"Atif Saleem Siddiqui\",\"doi\":\"10.1002/ccr3.9595\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 19-year-old male with no known medical comorbidities presented to the emergency department with a dry cough and shortness of breath for 3 months. His heart rate was 114/min, respiratory rate was 32/min, blood pressure was 110/80 mmHg, temperature was 101.5 °F, and oxygen saturation was 86% on room air. Initial laboratory data were normal, and a serum Quantiferon test was positive. Computed tomography (CT) of the chest showed bilateral diffuse miliary infiltrates and ground-glass opacities (GGO), with mild bronchiectasis in the left upper lobe (Figure 1A). He required heated high-flow oxygen in the emergency department; however, he was intubated due to worsening respiratory failure and increased work of breathing. Bronchoscopy with bronchoalveolar lavage (BAL) was performed. BAL and tracheal aspirates were negative for <i>Mycobacterium tuberculosis</i> (MTB) polymerase chain reaction (PCR), acid-fast bacilli (AFB), bacterial, and fungal cultures. He remained on mechanical ventilation for 1 week, and all his cultures were negative. A second bronchoscopy with transbronchial cryobiopsy (TBLC) was performed to obtain a tissue diagnosis. TBLC revealed caseating granulomas and multinucleated giant cells (Figure 1B). Grocott's methenamine silver stain was negative. Tissue AFB cultures and MTB PCR obtained via TBLC came back positive for tuberculosis within 1 week. The patient was started on rifampin, isoniazid, pyrazinamide, and ethambutol for a 6-month course. He required a tracheostomy 16 days after mechanical ventilation and was able to wean off mechanical ventilation, being successfully decannulated 2 weeks after the tracheostomy.</p><p>Miliary tuberculosis is a life-threatening hematogenous dissemination of <i>Mycobacterium tuberculosis</i> bacilli. The diagnosis of pulmonary tuberculosis is determined by symptoms, risk factors, sputum smear microscopy, and chest radiography. In miliary TB, acid-fast bacilli (AFB) smears are positive in only 20%–25% of cases, and cultures of sputum are positive in 30%–65% of patients [<span>1</span>]. Transbronchial biopsy diagnostic yields are 62.5%–76% [<span>2</span>]. TBLC has been widely used for the diagnosis of interstitial lung disease. However, the role of TBLC in the diagnosis of culture-negative miliary TB remains unclear. There is limited data on the use of TBLC in culture-negative miliary TB. A case report by Nasu et al. [<span>3</span>] demonstrated the utility of TBLC in diagnosing miliary tuberculosis that initially mimicked hypersensitivity pneumonitis. In this case, cryobiopsy specimens revealed necrotic granulomas, which led to a re-examination of sputum and subsequent identification of <i>Mycobacterium tuberculosis</i>. The patient described in our case had ground-glass opacities (GGO), a rare presentation of miliary TB. Furthermore, sputum and BAL AFB cultures, as well as MTB PCR, were negative. Additionally, Sánchez-Cabral et al. highlighted the diagnostic value of TBLC in non-interstitial lung diseases, including infectious diseases like TB. The study reported a high diagnostic yield when TBLC was combined with bronchoalveolar lavage (BAL), suggesting that TBLC can be a robust diagnostic tool in cases where traditional methods are inconclusive. This case contributes to the limited pool of literature, highlighting the use of TBLC in miliary TB in patients with negative BAL and tracheal aspirates. Furthermore, GGO is an uncommon CT chest characteristic of disseminated TB and can be associated with serious complications. In conclusion, further studies are needed to determine the utility and diagnostic yield of TBLC in this patient population.</p><p><b>Atif Saleem Siddiqui:</b> conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualization, writing – original draft, writing – review and editing.</p><p>Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.</p><p>The author declares no conflicts of interest.</p>\",\"PeriodicalId\":10327,\"journal\":{\"name\":\"Clinical Case Reports\",\"volume\":\"12 11\",\"pages\":\"\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-11-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccr3.9595\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ccr3.9595\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccr3.9595","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Transbronchial Cryobiopsy for the Diagnosis of Culture Negative Miliary Tuberculosis
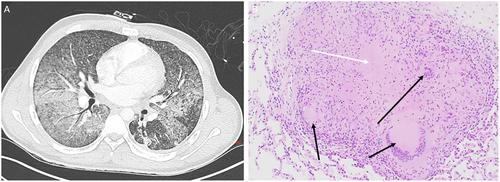
A 19-year-old male with no known medical comorbidities presented to the emergency department with a dry cough and shortness of breath for 3 months. His heart rate was 114/min, respiratory rate was 32/min, blood pressure was 110/80 mmHg, temperature was 101.5 °F, and oxygen saturation was 86% on room air. Initial laboratory data were normal, and a serum Quantiferon test was positive. Computed tomography (CT) of the chest showed bilateral diffuse miliary infiltrates and ground-glass opacities (GGO), with mild bronchiectasis in the left upper lobe (Figure 1A). He required heated high-flow oxygen in the emergency department; however, he was intubated due to worsening respiratory failure and increased work of breathing. Bronchoscopy with bronchoalveolar lavage (BAL) was performed. BAL and tracheal aspirates were negative for Mycobacterium tuberculosis (MTB) polymerase chain reaction (PCR), acid-fast bacilli (AFB), bacterial, and fungal cultures. He remained on mechanical ventilation for 1 week, and all his cultures were negative. A second bronchoscopy with transbronchial cryobiopsy (TBLC) was performed to obtain a tissue diagnosis. TBLC revealed caseating granulomas and multinucleated giant cells (Figure 1B). Grocott's methenamine silver stain was negative. Tissue AFB cultures and MTB PCR obtained via TBLC came back positive for tuberculosis within 1 week. The patient was started on rifampin, isoniazid, pyrazinamide, and ethambutol for a 6-month course. He required a tracheostomy 16 days after mechanical ventilation and was able to wean off mechanical ventilation, being successfully decannulated 2 weeks after the tracheostomy.
Miliary tuberculosis is a life-threatening hematogenous dissemination of Mycobacterium tuberculosis bacilli. The diagnosis of pulmonary tuberculosis is determined by symptoms, risk factors, sputum smear microscopy, and chest radiography. In miliary TB, acid-fast bacilli (AFB) smears are positive in only 20%–25% of cases, and cultures of sputum are positive in 30%–65% of patients [1]. Transbronchial biopsy diagnostic yields are 62.5%–76% [2]. TBLC has been widely used for the diagnosis of interstitial lung disease. However, the role of TBLC in the diagnosis of culture-negative miliary TB remains unclear. There is limited data on the use of TBLC in culture-negative miliary TB. A case report by Nasu et al. [3] demonstrated the utility of TBLC in diagnosing miliary tuberculosis that initially mimicked hypersensitivity pneumonitis. In this case, cryobiopsy specimens revealed necrotic granulomas, which led to a re-examination of sputum and subsequent identification of Mycobacterium tuberculosis. The patient described in our case had ground-glass opacities (GGO), a rare presentation of miliary TB. Furthermore, sputum and BAL AFB cultures, as well as MTB PCR, were negative. Additionally, Sánchez-Cabral et al. highlighted the diagnostic value of TBLC in non-interstitial lung diseases, including infectious diseases like TB. The study reported a high diagnostic yield when TBLC was combined with bronchoalveolar lavage (BAL), suggesting that TBLC can be a robust diagnostic tool in cases where traditional methods are inconclusive. This case contributes to the limited pool of literature, highlighting the use of TBLC in miliary TB in patients with negative BAL and tracheal aspirates. Furthermore, GGO is an uncommon CT chest characteristic of disseminated TB and can be associated with serious complications. In conclusion, further studies are needed to determine the utility and diagnostic yield of TBLC in this patient population.
Atif Saleem Siddiqui: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualization, writing – original draft, writing – review and editing.
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
期刊介绍:
Clinical Case Reports is different from other case report journals. Our aim is to directly improve global health and increase clinical understanding using case reports to convey important best practice information. We welcome case reports from all areas of Medicine, Nursing, Dentistry, and Veterinary Science and may include: -Any clinical case or procedure which illustrates an important best practice teaching message -Any clinical case or procedure which illustrates the appropriate use of an important clinical guideline or systematic review. As well as: -The management of novel or very uncommon diseases -A common disease presenting in an uncommon way -An uncommon disease masquerading as something more common -Cases which expand understanding of disease pathogenesis -Cases where the teaching point is based on an error -Cases which allow us to re-think established medical lore -Unreported adverse effects of interventions (drug, procedural, or other).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
