Markku Grönroos, Ville Hällberg, Mika Helminen, Teemu Koivistoinen, Ari Palomäki
{"title":"使用统计过程控制图分析急性缺血性脑卒中溶栓治疗从进门到进针的时间。","authors":"Markku Grönroos, Ville Hällberg, Mika Helminen, Teemu Koivistoinen, Ari Palomäki","doi":"10.1136/bmjno-2024-000687","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thrombolysis should be administered as soon as possible to suitable patients with acute ischaemic stroke. We introduced a new protocol for patients who had a stroke to achieve reduced door-to-needle times for the best possible outcome. Since then, we have closely monitored each patient who had a stroke. Our goal was to assess whether statistical process control charts could be useful in detecting deviations in door-to-needle times when using four well-known rules applied by Western Electric (WE rules 1-4).</p><p><strong>Methods: </strong>We analysed retrospectively door-to-needle times of together 200 acute ischaemic stroke patients before and after the implementation of our new stroke protocol. In addition, 25 patients at the time of reorganisation (transition period) were analysed. Statistical process control chart rules WE 1-WE 4 were applied to detect door-to-needle deviations and to monitor process uniformity.</p><p><strong>Results: </strong>Before the implementation of the protocol, median door-to-needle time was 53 min and after the implementation 20 min. Statistical process control chart rules were triggered only once in 100 patients before the reorganisation but seven times in 25 patients during the transition period. None of the rules WE 1-4 were activated after the reorganisation, indicating the stability of the reorganised acute ischaemic stroke process.</p><p><strong>Conclusions: </strong>The use of statistical process control charts demonstrated a significant reduction in door-to-needle times during the reorganisation. Further, it showed that the acute ischaemic stroke process with a 20 min door-to-needle time is very stable.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"6 2","pages":"e000687"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11575376/pdf/","citationCount":"0","resultStr":"{\"title\":\"Analysis of door-to-needle time for thrombolysis in acute ischaemic stroke using statistical process control charts.\",\"authors\":\"Markku Grönroos, Ville Hällberg, Mika Helminen, Teemu Koivistoinen, Ari Palomäki\",\"doi\":\"10.1136/bmjno-2024-000687\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Thrombolysis should be administered as soon as possible to suitable patients with acute ischaemic stroke. We introduced a new protocol for patients who had a stroke to achieve reduced door-to-needle times for the best possible outcome. Since then, we have closely monitored each patient who had a stroke. Our goal was to assess whether statistical process control charts could be useful in detecting deviations in door-to-needle times when using four well-known rules applied by Western Electric (WE rules 1-4).</p><p><strong>Methods: </strong>We analysed retrospectively door-to-needle times of together 200 acute ischaemic stroke patients before and after the implementation of our new stroke protocol. In addition, 25 patients at the time of reorganisation (transition period) were analysed. Statistical process control chart rules WE 1-WE 4 were applied to detect door-to-needle deviations and to monitor process uniformity.</p><p><strong>Results: </strong>Before the implementation of the protocol, median door-to-needle time was 53 min and after the implementation 20 min. Statistical process control chart rules were triggered only once in 100 patients before the reorganisation but seven times in 25 patients during the transition period. None of the rules WE 1-4 were activated after the reorganisation, indicating the stability of the reorganised acute ischaemic stroke process.</p><p><strong>Conclusions: </strong>The use of statistical process control charts demonstrated a significant reduction in door-to-needle times during the reorganisation. Further, it showed that the acute ischaemic stroke process with a 20 min door-to-needle time is very stable.</p>\",\"PeriodicalId\":52754,\"journal\":{\"name\":\"BMJ Neurology Open\",\"volume\":\"6 2\",\"pages\":\"e000687\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-11-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11575376/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Neurology Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjno-2024-000687\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2024-000687","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Analysis of door-to-needle time for thrombolysis in acute ischaemic stroke using statistical process control charts.
Background: Thrombolysis should be administered as soon as possible to suitable patients with acute ischaemic stroke. We introduced a new protocol for patients who had a stroke to achieve reduced door-to-needle times for the best possible outcome. Since then, we have closely monitored each patient who had a stroke. Our goal was to assess whether statistical process control charts could be useful in detecting deviations in door-to-needle times when using four well-known rules applied by Western Electric (WE rules 1-4).
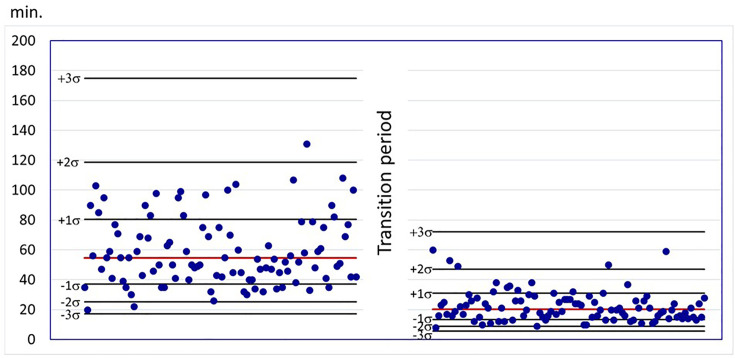
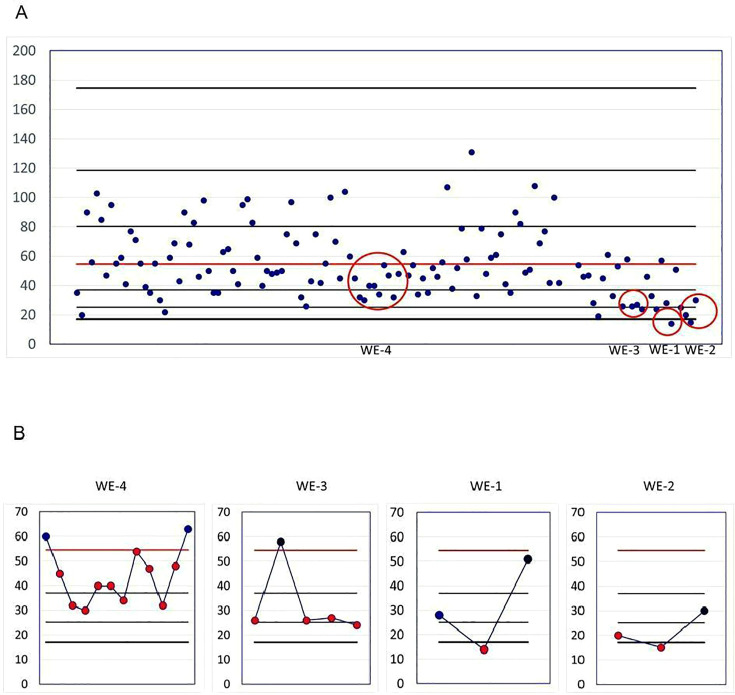
Methods: We analysed retrospectively door-to-needle times of together 200 acute ischaemic stroke patients before and after the implementation of our new stroke protocol. In addition, 25 patients at the time of reorganisation (transition period) were analysed. Statistical process control chart rules WE 1-WE 4 were applied to detect door-to-needle deviations and to monitor process uniformity.
Results: Before the implementation of the protocol, median door-to-needle time was 53 min and after the implementation 20 min. Statistical process control chart rules were triggered only once in 100 patients before the reorganisation but seven times in 25 patients during the transition period. None of the rules WE 1-4 were activated after the reorganisation, indicating the stability of the reorganised acute ischaemic stroke process.
Conclusions: The use of statistical process control charts demonstrated a significant reduction in door-to-needle times during the reorganisation. Further, it showed that the acute ischaemic stroke process with a 20 min door-to-needle time is very stable.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
