Janine B Kastelijn, A Merel van den Berg, Raju Talwar, Marije S Koks, Marije Marsman, Karel J van Erpecum, Paul Didden, Leon M G Moons, Frank P Vleggaar
{"title":"使用异丙酚深度镇静的内镜逆行胰胆管造影术的技术成功率和不良事件发生率。","authors":"Janine B Kastelijn, A Merel van den Berg, Raju Talwar, Marije S Koks, Marije Marsman, Karel J van Erpecum, Paul Didden, Leon M G Moons, Frank P Vleggaar","doi":"10.20524/aog.2024.0925","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>With the increasing complexity and prolonged duration of endoscopic retrograde cholangiopancreatography (ERCP) procedures, sedation shifted from conscious sedation with benzodiazepines to deep sedation with propofol. We assessed the technical success and adverse event rates of ERCP with deep versus conscious sedation.</p><p><strong>Methods: </strong>Consecutive patients treated with ERCP in the University Medical Center Utrecht over a 7-year period (2010-2016) were screened for eligibility. Gastroenterologist-administered conscious sedation with midazolam was used from 2010-2013, whilst anesthesiology-administered deep sedation with propofol was used from 2013-2016. Data were retrospectively collected from electronic medical records. Outcomes were technical success and procedure-related adverse events within 30 days after ERCP. Associations of sedation type with outcomes were analyzed in univariable and multivariable analyses.</p><p><strong>Results: </strong>A total of 725 patients were included: 336 (46%) with conscious sedation and 389 (54%) with deep sedation. Technical success was significantly higher when propofol-based sedation was used (317 [82%] vs. 252 [75%], P=0.034). Adverse events also occurred significantly more often in the propofol group (77 [20%] vs. 38 [11%], P=0.002), due to higher rates of post-ERCP cholangitis (21 [5%] vs. 8 [2%], P=0.039), and post-ERCP pancreatitis (29 [7%] vs. 11 [3%], P=0.014). After adjustment, propofol-based sedation remained significantly associated with technical success and adverse events, with odds ratios of 1.53 (95% confidence interval [CI] 1.05-2.21) and 1.95 (95% CI 1.25-3.04), respectively.</p><p><strong>Conclusion: </strong>Propofol-based sedation resulted significantly more often in technical success of ERCP compared with midazolam-based sedation, but adverse events were almost twice as common, with higher rates of post-ERCP pancreatitis and cholangitis.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 6","pages":"726-733"},"PeriodicalIF":2.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574159/pdf/","citationCount":"0","resultStr":"{\"title\":\"Technical success and adverse event rates after endoscopic retrograde cholangiopancreatography using deep sedation with propofol.\",\"authors\":\"Janine B Kastelijn, A Merel van den Berg, Raju Talwar, Marije S Koks, Marije Marsman, Karel J van Erpecum, Paul Didden, Leon M G Moons, Frank P Vleggaar\",\"doi\":\"10.20524/aog.2024.0925\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>With the increasing complexity and prolonged duration of endoscopic retrograde cholangiopancreatography (ERCP) procedures, sedation shifted from conscious sedation with benzodiazepines to deep sedation with propofol. We assessed the technical success and adverse event rates of ERCP with deep versus conscious sedation.</p><p><strong>Methods: </strong>Consecutive patients treated with ERCP in the University Medical Center Utrecht over a 7-year period (2010-2016) were screened for eligibility. Gastroenterologist-administered conscious sedation with midazolam was used from 2010-2013, whilst anesthesiology-administered deep sedation with propofol was used from 2013-2016. Data were retrospectively collected from electronic medical records. Outcomes were technical success and procedure-related adverse events within 30 days after ERCP. Associations of sedation type with outcomes were analyzed in univariable and multivariable analyses.</p><p><strong>Results: </strong>A total of 725 patients were included: 336 (46%) with conscious sedation and 389 (54%) with deep sedation. Technical success was significantly higher when propofol-based sedation was used (317 [82%] vs. 252 [75%], P=0.034). Adverse events also occurred significantly more often in the propofol group (77 [20%] vs. 38 [11%], P=0.002), due to higher rates of post-ERCP cholangitis (21 [5%] vs. 8 [2%], P=0.039), and post-ERCP pancreatitis (29 [7%] vs. 11 [3%], P=0.014). After adjustment, propofol-based sedation remained significantly associated with technical success and adverse events, with odds ratios of 1.53 (95% confidence interval [CI] 1.05-2.21) and 1.95 (95% CI 1.25-3.04), respectively.</p><p><strong>Conclusion: </strong>Propofol-based sedation resulted significantly more often in technical success of ERCP compared with midazolam-based sedation, but adverse events were almost twice as common, with higher rates of post-ERCP pancreatitis and cholangitis.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"37 6\",\"pages\":\"726-733\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574159/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2024.0925\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0925","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:随着内镜逆行胰胆管造影术(ERCP)的复杂性增加和持续时间延长,镇静方式从使用苯二氮卓类药物的清醒镇静转变为使用异丙酚的深度镇静。我们评估了深度镇静与清醒镇静ERCP的技术成功率和不良事件发生率:筛选了乌得勒支大学医学中心在 7 年内(2010-2016 年)接受 ERCP 治疗的连续患者。2010-2013年期间,消化内科医生使用咪达唑仑进行有意识镇静,2013-2016年期间,麻醉科使用异丙酚进行深度镇静。数据通过电子病历进行回顾性收集。结果为ERCP术后30天内的技术成功率和手术相关不良事件。通过单变量和多变量分析分析了镇静类型与结果的相关性:结果:共纳入 725 名患者:结果:共纳入 725 例患者:336 例(46%)采用意识镇静,389 例(54%)采用深度镇静。使用异丙酚镇静时,技术成功率明显更高(317 [82%] 对 252 [75%],P=0.034)。异丙酚组的不良事件发生率也明显更高(77 [20%] vs. 38 [11%],P=0.002),这是因为异丙酚术后胆管炎(21 [5%] vs. 8 [2%],P=0.039)和异丙酚术后胰腺炎(29 [7%] vs. 11 [3%],P=0.014)的发生率更高。经调整后,异丙酚镇静仍与技术成功率和不良事件显著相关,几率比分别为 1.53(95% 置信区间 [CI] 1.05-2.21)和 1.95(95% CI 1.25-3.04):结论:与咪达唑仑镇静法相比,丙泊酚镇静法可显著提高ERCP的技术成功率,但不良事件的发生率几乎是咪达唑仑镇静法的两倍,ERCP术后胰腺炎和胆管炎的发生率更高。
Technical success and adverse event rates after endoscopic retrograde cholangiopancreatography using deep sedation with propofol.
Background: With the increasing complexity and prolonged duration of endoscopic retrograde cholangiopancreatography (ERCP) procedures, sedation shifted from conscious sedation with benzodiazepines to deep sedation with propofol. We assessed the technical success and adverse event rates of ERCP with deep versus conscious sedation.
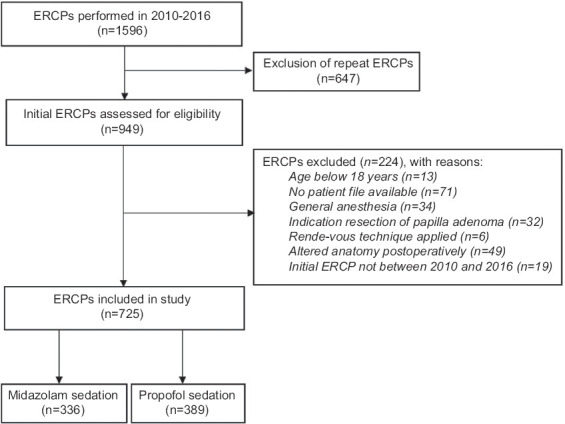
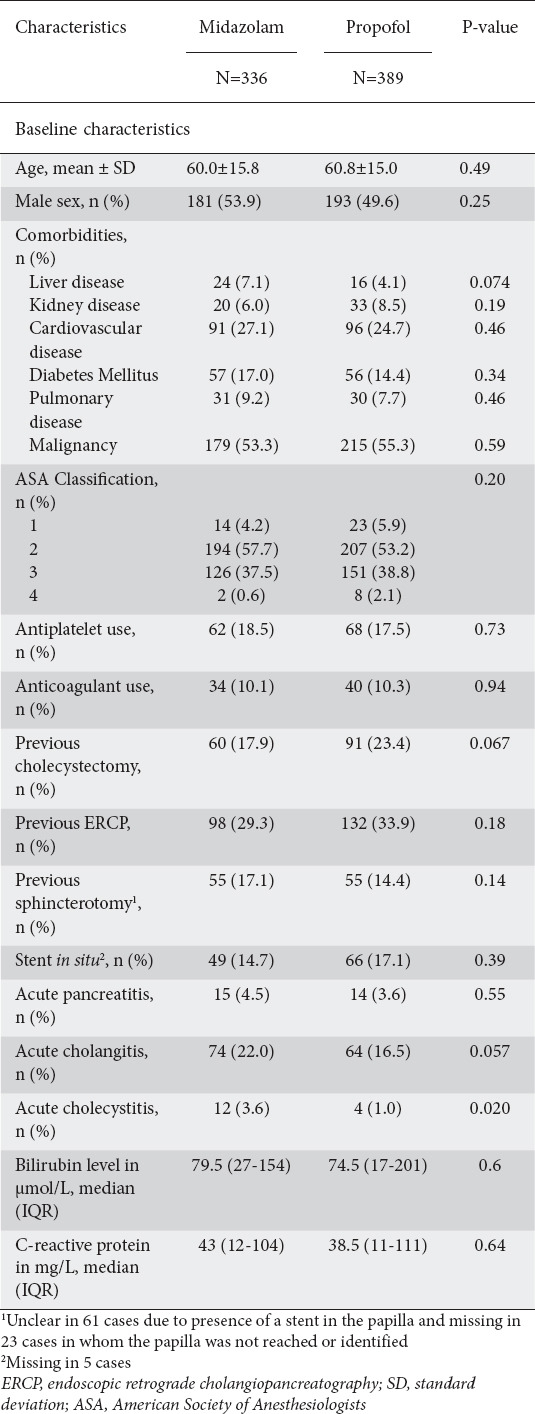
Methods: Consecutive patients treated with ERCP in the University Medical Center Utrecht over a 7-year period (2010-2016) were screened for eligibility. Gastroenterologist-administered conscious sedation with midazolam was used from 2010-2013, whilst anesthesiology-administered deep sedation with propofol was used from 2013-2016. Data were retrospectively collected from electronic medical records. Outcomes were technical success and procedure-related adverse events within 30 days after ERCP. Associations of sedation type with outcomes were analyzed in univariable and multivariable analyses.
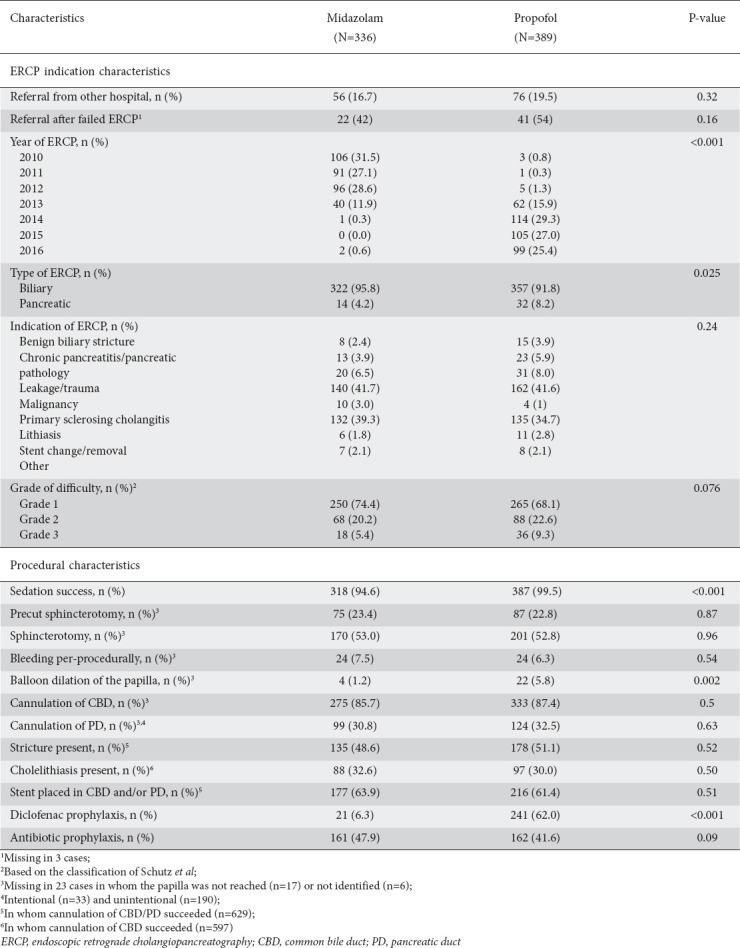
Results: A total of 725 patients were included: 336 (46%) with conscious sedation and 389 (54%) with deep sedation. Technical success was significantly higher when propofol-based sedation was used (317 [82%] vs. 252 [75%], P=0.034). Adverse events also occurred significantly more often in the propofol group (77 [20%] vs. 38 [11%], P=0.002), due to higher rates of post-ERCP cholangitis (21 [5%] vs. 8 [2%], P=0.039), and post-ERCP pancreatitis (29 [7%] vs. 11 [3%], P=0.014). After adjustment, propofol-based sedation remained significantly associated with technical success and adverse events, with odds ratios of 1.53 (95% confidence interval [CI] 1.05-2.21) and 1.95 (95% CI 1.25-3.04), respectively.
Conclusion: Propofol-based sedation resulted significantly more often in technical success of ERCP compared with midazolam-based sedation, but adverse events were almost twice as common, with higher rates of post-ERCP pancreatitis and cholangitis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
