Kristina K M Kramer, Nina-Sophie Schmidt-Hegemann, Thilo Westhofen, Marco Foglar, Jens Ricke, C Benedikt Westphalen, Marcus Unterrainer, Wolfgang G Kunz, Dirk Mehrens
{"title":"从医疗保险的角度分析转移性前列腺癌局部前列腺放射治疗的成本效益。","authors":"Kristina K M Kramer, Nina-Sophie Schmidt-Hegemann, Thilo Westhofen, Marco Foglar, Jens Ricke, C Benedikt Westphalen, Marcus Unterrainer, Wolfgang G Kunz, Dirk Mehrens","doi":"10.1186/s13014-024-02544-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Metastatic prostate cancer remains a therapeutic challenge. Based on data of the STAMPEDE trial, patients with a low metastatic burden showed prolonged failure-free and overall survival when treated with prostate radio therapy (RT) in addition to standard of care (SOC). The objective of this study was to determine the cost-effectiveness of additional prostate RT compared to SOC alone for following subgroups: non-regional lymph node (NRLN) metastases, up to three bone metastases and four or more bone metastases.</p><p><strong>Methods: </strong>A partitioned survival model was implemented with clinical data from STAMPEDE trial. Analyses were performed from a United States healthcare system perspective. Costs for treatment and adverse events were derived from Medicare coverage. Utilities for health states were derived from public databases and literature. Outcome measurements included incremental costs, effectiveness, and cost-effectiveness ratio. The willingness-to-pay threshold was set to USD 100,000 per quality-adjusted life year (QALY).</p><p><strong>Results: </strong>Additional RT led to 0.92 incremental QALYs with increased costs of USD 26,098 with an incremental cost-effectiveness ratio (ICER) of USD 28,452/QALY for patients with only NRLN metastases and 3.83 incremental QALYs with increased costs of USD 153,490 with an ICER of USD 40,032/QALY for patients with up to three bone metastases. Sensitivity analysis showed robustness of the model regarding various parameters. In probabilistic sensitivity analysis using Monte Carlo simulation with 10,000 iterations, additional RT was found as the cost-effective strategy in over 96% for both subgroups iterations at a willingness-to-pay threshold of USD 100,000/QALYs.</p><p><strong>Conclusions: </strong>Additional RT is cost-effective in patients with only NRLN metastases and up to three metastases compared to SOC.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"19 1","pages":"167"},"PeriodicalIF":3.3000,"publicationDate":"2024-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11580356/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness analysis of additional local prostate radio therapy in metastatic prostate cancer from a medicare perspective.\",\"authors\":\"Kristina K M Kramer, Nina-Sophie Schmidt-Hegemann, Thilo Westhofen, Marco Foglar, Jens Ricke, C Benedikt Westphalen, Marcus Unterrainer, Wolfgang G Kunz, Dirk Mehrens\",\"doi\":\"10.1186/s13014-024-02544-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Metastatic prostate cancer remains a therapeutic challenge. Based on data of the STAMPEDE trial, patients with a low metastatic burden showed prolonged failure-free and overall survival when treated with prostate radio therapy (RT) in addition to standard of care (SOC). The objective of this study was to determine the cost-effectiveness of additional prostate RT compared to SOC alone for following subgroups: non-regional lymph node (NRLN) metastases, up to three bone metastases and four or more bone metastases.</p><p><strong>Methods: </strong>A partitioned survival model was implemented with clinical data from STAMPEDE trial. Analyses were performed from a United States healthcare system perspective. Costs for treatment and adverse events were derived from Medicare coverage. Utilities for health states were derived from public databases and literature. Outcome measurements included incremental costs, effectiveness, and cost-effectiveness ratio. The willingness-to-pay threshold was set to USD 100,000 per quality-adjusted life year (QALY).</p><p><strong>Results: </strong>Additional RT led to 0.92 incremental QALYs with increased costs of USD 26,098 with an incremental cost-effectiveness ratio (ICER) of USD 28,452/QALY for patients with only NRLN metastases and 3.83 incremental QALYs with increased costs of USD 153,490 with an ICER of USD 40,032/QALY for patients with up to three bone metastases. Sensitivity analysis showed robustness of the model regarding various parameters. In probabilistic sensitivity analysis using Monte Carlo simulation with 10,000 iterations, additional RT was found as the cost-effective strategy in over 96% for both subgroups iterations at a willingness-to-pay threshold of USD 100,000/QALYs.</p><p><strong>Conclusions: </strong>Additional RT is cost-effective in patients with only NRLN metastases and up to three metastases compared to SOC.</p>\",\"PeriodicalId\":49639,\"journal\":{\"name\":\"Radiation Oncology\",\"volume\":\"19 1\",\"pages\":\"167\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-11-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11580356/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13014-024-02544-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-024-02544-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Cost-effectiveness analysis of additional local prostate radio therapy in metastatic prostate cancer from a medicare perspective.
Background: Metastatic prostate cancer remains a therapeutic challenge. Based on data of the STAMPEDE trial, patients with a low metastatic burden showed prolonged failure-free and overall survival when treated with prostate radio therapy (RT) in addition to standard of care (SOC). The objective of this study was to determine the cost-effectiveness of additional prostate RT compared to SOC alone for following subgroups: non-regional lymph node (NRLN) metastases, up to three bone metastases and four or more bone metastases.
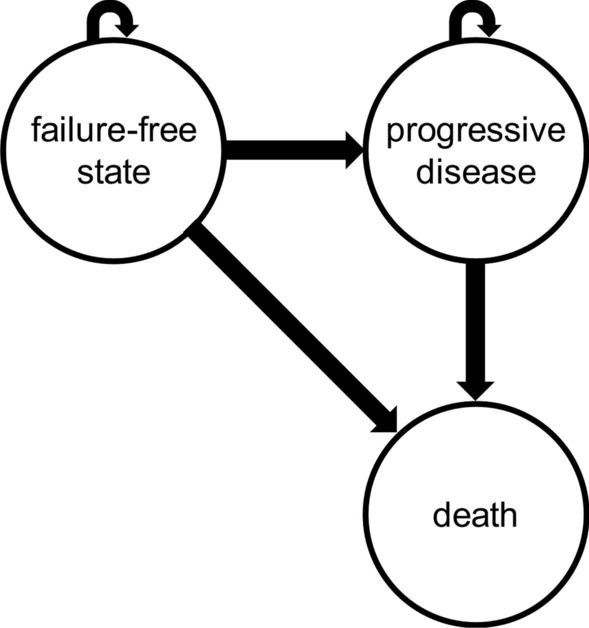
Methods: A partitioned survival model was implemented with clinical data from STAMPEDE trial. Analyses were performed from a United States healthcare system perspective. Costs for treatment and adverse events were derived from Medicare coverage. Utilities for health states were derived from public databases and literature. Outcome measurements included incremental costs, effectiveness, and cost-effectiveness ratio. The willingness-to-pay threshold was set to USD 100,000 per quality-adjusted life year (QALY).
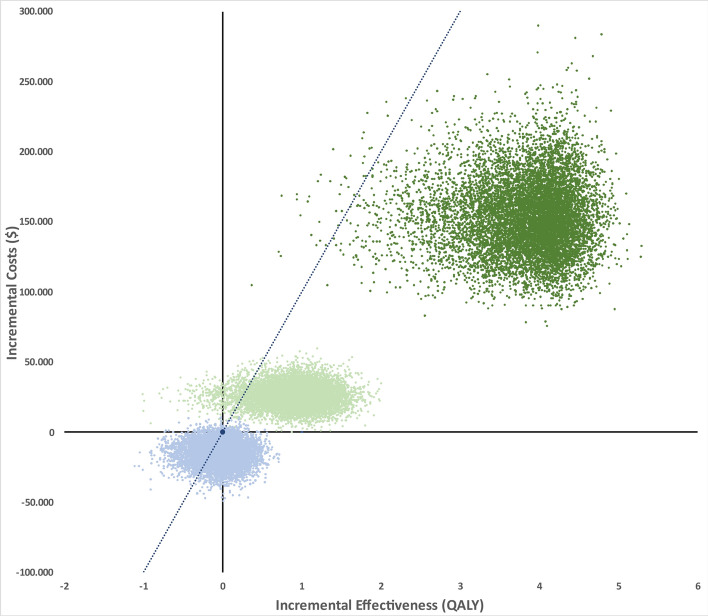
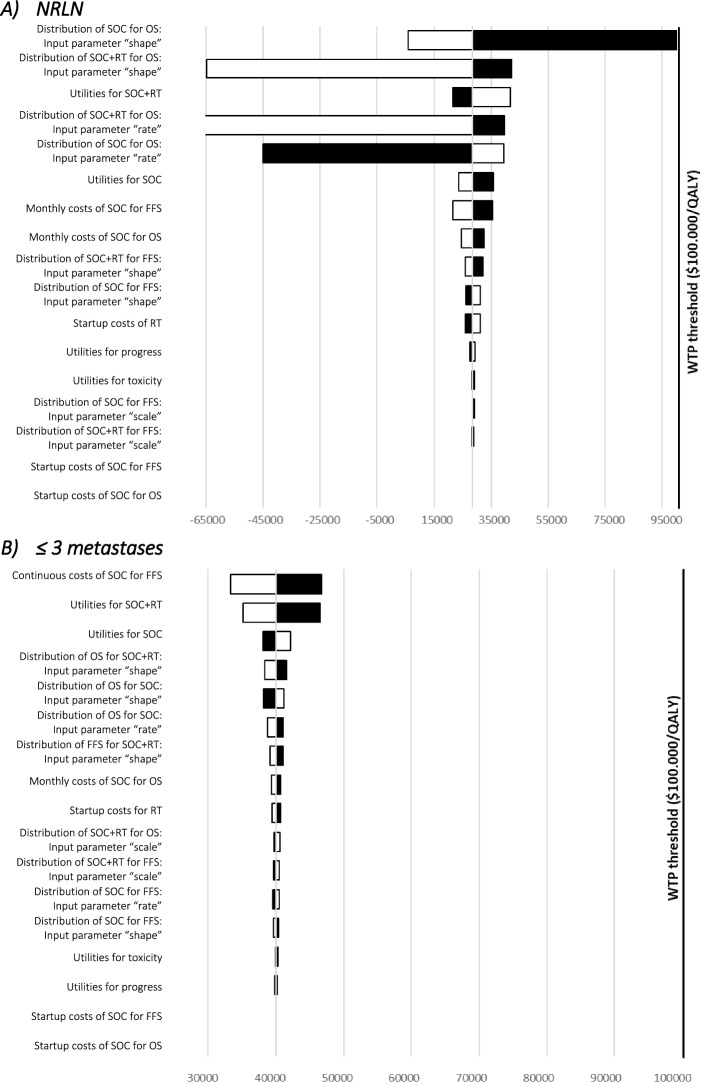
Results: Additional RT led to 0.92 incremental QALYs with increased costs of USD 26,098 with an incremental cost-effectiveness ratio (ICER) of USD 28,452/QALY for patients with only NRLN metastases and 3.83 incremental QALYs with increased costs of USD 153,490 with an ICER of USD 40,032/QALY for patients with up to three bone metastases. Sensitivity analysis showed robustness of the model regarding various parameters. In probabilistic sensitivity analysis using Monte Carlo simulation with 10,000 iterations, additional RT was found as the cost-effective strategy in over 96% for both subgroups iterations at a willingness-to-pay threshold of USD 100,000/QALYs.
Conclusions: Additional RT is cost-effective in patients with only NRLN metastases and up to three metastases compared to SOC.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
