Marion Morena-Carrere, Isabelle Jaussent, Leila Chenine, Anne-Marie Dupuy, Anne-Sophie Bargnoux, Hélène Leray-Moragues, Kada Klouche, Hélène Vernhet, Bernard Canaud, Jean-Paul Cristol
{"title":"慢性肾病患者严重的冠状动脉钙化,再加上炎症和骨矿物质疾病的失调,会通过血管重塑促进重大不良心血管事件(MACE)的发生。","authors":"Marion Morena-Carrere, Isabelle Jaussent, Leila Chenine, Anne-Marie Dupuy, Anne-Sophie Bargnoux, Hélène Leray-Moragues, Kada Klouche, Hélène Vernhet, Bernard Canaud, Jean-Paul Cristol","doi":"10.1159/000542418","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cardiovascular (CV) diseases persist as the foremost cause of morbidity/mortality among chronic kidney disease (CKD) patients. This paper examines the values of coronary artery calcification (CAC) and biomarkers of CV on major adverse CV events (MACE)/CV death in a sample of 425 non-dialysis CKD patients.</p><p><strong>Methods: </strong>At inclusion, patients underwent chest multidetector computed tomography for CAC scoring and biomarkers of CV risk including CRP, mineral metabolism markers, fibroblast growth factor-23 (FGF-23), α-Klotho, osteoprotegerin, tartrate-resistant acid phosphatase 5b (TRAP5b), sclerostin, matrix gla protein (both dephosphorylated uncarboxylated [dp-ucMGP] and total uncarboxylated), and growth differentiation factor-15 (GDF-15) were measured. Patients were followed for a median of 3.61 years (25th-75th percentiles = 1.92-6.70).</p><p><strong>Results: </strong>Our results reported that CAC was a major independent factor of MACE/CV mortality showing a hazard ratio of 1.71 95% (confidence interval = 1.00-2.93) after adjustment for age, gender, diabetes, and history of CV events for patients with CAC >300. Interestingly, CAC effect was further enhanced in the presence of low levels of 25(OH) vitamin D3 or α-Klotho and high levels of intact parathyroid hormone (PTH), high-sensitive C reactive protein, FGF-23, osteoprotegerin, sclerostin, dp-ucMGP, or GDF-15.</p><p><strong>Conclusion: </strong>CAC constitutes a significant CV risk, further exacerbated by inflammation, hyperparathyroidism, and regulation of bone molecules implicated in calcification progression. This finding aligns with the original concept of multiple hits. Consequently, addressing the detrimental environment that fosters plaque vulnerability, reducing chronic low-grade inflammation, and normalizing mineral metabolism markers (such as vitamin D and PTH) and bone-regulating molecules may emerge as a viable therapeutic strategy.</p>","PeriodicalId":17813,"journal":{"name":"Kidney & blood pressure research","volume":" ","pages":"33-45"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844697/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe Coronary Artery Calcifications in Chronic Kidney Disease Patients, Coupled with Inflammation and Bone Mineral Disease Derangement, Promote Major Adverse Cardiovascular Events through Vascular Remodeling.\",\"authors\":\"Marion Morena-Carrere, Isabelle Jaussent, Leila Chenine, Anne-Marie Dupuy, Anne-Sophie Bargnoux, Hélène Leray-Moragues, Kada Klouche, Hélène Vernhet, Bernard Canaud, Jean-Paul Cristol\",\"doi\":\"10.1159/000542418\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cardiovascular (CV) diseases persist as the foremost cause of morbidity/mortality among chronic kidney disease (CKD) patients. This paper examines the values of coronary artery calcification (CAC) and biomarkers of CV on major adverse CV events (MACE)/CV death in a sample of 425 non-dialysis CKD patients.</p><p><strong>Methods: </strong>At inclusion, patients underwent chest multidetector computed tomography for CAC scoring and biomarkers of CV risk including CRP, mineral metabolism markers, fibroblast growth factor-23 (FGF-23), α-Klotho, osteoprotegerin, tartrate-resistant acid phosphatase 5b (TRAP5b), sclerostin, matrix gla protein (both dephosphorylated uncarboxylated [dp-ucMGP] and total uncarboxylated), and growth differentiation factor-15 (GDF-15) were measured. Patients were followed for a median of 3.61 years (25th-75th percentiles = 1.92-6.70).</p><p><strong>Results: </strong>Our results reported that CAC was a major independent factor of MACE/CV mortality showing a hazard ratio of 1.71 95% (confidence interval = 1.00-2.93) after adjustment for age, gender, diabetes, and history of CV events for patients with CAC >300. Interestingly, CAC effect was further enhanced in the presence of low levels of 25(OH) vitamin D3 or α-Klotho and high levels of intact parathyroid hormone (PTH), high-sensitive C reactive protein, FGF-23, osteoprotegerin, sclerostin, dp-ucMGP, or GDF-15.</p><p><strong>Conclusion: </strong>CAC constitutes a significant CV risk, further exacerbated by inflammation, hyperparathyroidism, and regulation of bone molecules implicated in calcification progression. This finding aligns with the original concept of multiple hits. Consequently, addressing the detrimental environment that fosters plaque vulnerability, reducing chronic low-grade inflammation, and normalizing mineral metabolism markers (such as vitamin D and PTH) and bone-regulating molecules may emerge as a viable therapeutic strategy.</p>\",\"PeriodicalId\":17813,\"journal\":{\"name\":\"Kidney & blood pressure research\",\"volume\":\" \",\"pages\":\"33-45\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844697/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kidney & blood pressure research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000542418\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney & blood pressure research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000542418","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Severe Coronary Artery Calcifications in Chronic Kidney Disease Patients, Coupled with Inflammation and Bone Mineral Disease Derangement, Promote Major Adverse Cardiovascular Events through Vascular Remodeling.
Introduction: Cardiovascular (CV) diseases persist as the foremost cause of morbidity/mortality among chronic kidney disease (CKD) patients. This paper examines the values of coronary artery calcification (CAC) and biomarkers of CV on major adverse CV events (MACE)/CV death in a sample of 425 non-dialysis CKD patients.
Methods: At inclusion, patients underwent chest multidetector computed tomography for CAC scoring and biomarkers of CV risk including CRP, mineral metabolism markers, fibroblast growth factor-23 (FGF-23), α-Klotho, osteoprotegerin, tartrate-resistant acid phosphatase 5b (TRAP5b), sclerostin, matrix gla protein (both dephosphorylated uncarboxylated [dp-ucMGP] and total uncarboxylated), and growth differentiation factor-15 (GDF-15) were measured. Patients were followed for a median of 3.61 years (25th-75th percentiles = 1.92-6.70).
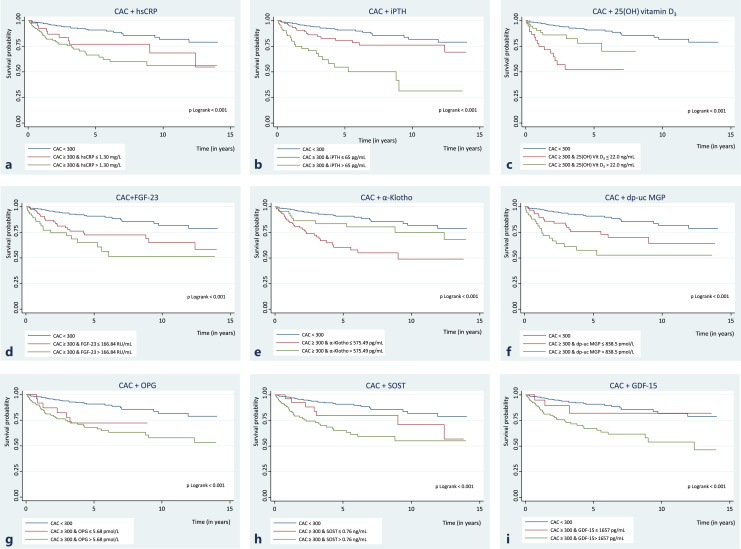
Results: Our results reported that CAC was a major independent factor of MACE/CV mortality showing a hazard ratio of 1.71 95% (confidence interval = 1.00-2.93) after adjustment for age, gender, diabetes, and history of CV events for patients with CAC >300. Interestingly, CAC effect was further enhanced in the presence of low levels of 25(OH) vitamin D3 or α-Klotho and high levels of intact parathyroid hormone (PTH), high-sensitive C reactive protein, FGF-23, osteoprotegerin, sclerostin, dp-ucMGP, or GDF-15.
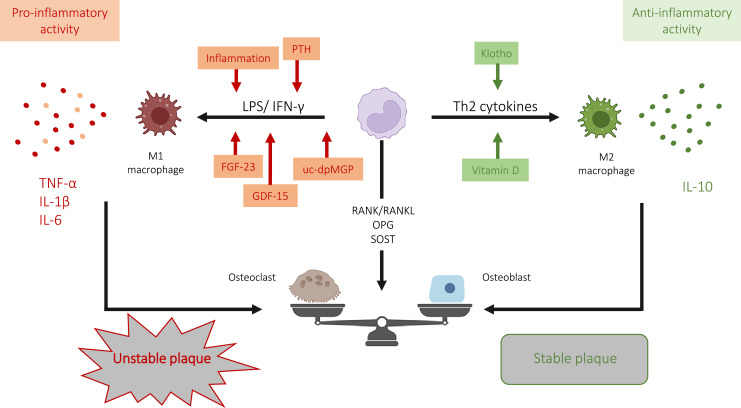
Conclusion: CAC constitutes a significant CV risk, further exacerbated by inflammation, hyperparathyroidism, and regulation of bone molecules implicated in calcification progression. This finding aligns with the original concept of multiple hits. Consequently, addressing the detrimental environment that fosters plaque vulnerability, reducing chronic low-grade inflammation, and normalizing mineral metabolism markers (such as vitamin D and PTH) and bone-regulating molecules may emerge as a viable therapeutic strategy.
期刊介绍:
This journal comprises both clinical and basic studies at the interface of nephrology, hypertension and cardiovascular research. The topics to be covered include the structural organization and biochemistry of the normal and diseased kidney, the molecular biology of transporters, the physiology and pathophysiology of glomerular filtration and tubular transport, endothelial and vascular smooth muscle cell function and blood pressure control, as well as water, electrolyte and mineral metabolism. Also discussed are the (patho)physiology and (patho) biochemistry of renal hormones, the molecular biology, genetics and clinical course of renal disease and hypertension, the renal elimination, action and clinical use of drugs, as well as dialysis and transplantation. Featuring peer-reviewed original papers, editorials translating basic science into patient-oriented research and disease, in depth reviews, and regular special topic sections, ''Kidney & Blood Pressure Research'' is an important source of information for researchers in nephrology and cardiovascular medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
