Ankur Mandelia, Rohit Kapoor, Anju Verma, Pujana Kanneganti, Rajanikant R Yadav, Moinak Sen Sarma, Nishant Agarwal, Tarun Kumar, Biju Nair, Amit Buan
{"title":"儿童胆总管囊肿的不同导管和血管解剖的腹腔镜治疗。","authors":"Ankur Mandelia, Rohit Kapoor, Anju Verma, Pujana Kanneganti, Rajanikant R Yadav, Moinak Sen Sarma, Nishant Agarwal, Tarun Kumar, Biju Nair, Amit Buan","doi":"10.4103/jmas.jmas_255_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Variations in biliary ductal and hepatic vascular anatomy increase the complexity of surgery for choledochal cysts (CDC). The laparoscopic approach for the management of paediatric CDCs with variant anatomy is underreported. This study aimed to describe anatomical variations, operative techniques and early outcomes of laparoscopic hepaticojejunostomy (HJ) in children with CDCs and variant anatomy.</p><p><strong>Patients and methods: </strong>We conducted a retrospective review of 40 children who underwent laparoscopic CDC excision with HJ between 2019 and 2024 in a single surgical unit. Patients were divided into Group I (with anatomical variations, n = 20) and Group II (without variations, n = 20). Data on demographic details, clinical presentation, imaging findings, pre-operative interventions, ductal and vascular anatomical variations, surgical techniques, intraoperative variables, post-operative complications and outcomes were collected and analysed.</p><p><strong>Results: </strong>Ductal variations were found in 10 patients, with aberrant right posterior sectoral duct being the most common. Vascular variations were identified in 12 patients, with anteriorly crossing the right hepatic artery (RHA) being the most frequent. Group I had a higher mean age (7.32 vs. 3.57 years, P = 0.014) and longer operative times (415 vs. 364 min, P < 0.0001). Conversion to laparotomy was necessary in 10% of Group I and 15% of Group II patients ( P = 0.634). Post-operative complications, primarily minor (Clavien-Dindo Grade I or II), occurred in 40% of Group I and 30% of Group II ( P = 0.495). Group I had a significantly shorter time to full feeds (72 vs. 80 h, P = 0.015). Both groups had similar post-operative hospital stays and follow-up durations. At the last follow-up, all patients, except one with liver failure in Group II, were asymptomatic with no significant biliary dilatation or liver function abnormalities.</p><p><strong>Conclusion: </strong>Laparoscopic management of CDCs with variant ductal and vascular anatomy in children is feasible, safe and effective. Detailed pre-operative imaging, meticulous intraoperative assessment and tailored surgical techniques are crucial for successful outcomes.</p>","PeriodicalId":48905,"journal":{"name":"Journal of Minimal Access Surgery","volume":" ","pages":"282-291"},"PeriodicalIF":1.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12327796/pdf/","citationCount":"0","resultStr":"{\"title\":\"Laparoscopic management of variant ductal and vascular anatomy in children with choledochal cysts.\",\"authors\":\"Ankur Mandelia, Rohit Kapoor, Anju Verma, Pujana Kanneganti, Rajanikant R Yadav, Moinak Sen Sarma, Nishant Agarwal, Tarun Kumar, Biju Nair, Amit Buan\",\"doi\":\"10.4103/jmas.jmas_255_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Variations in biliary ductal and hepatic vascular anatomy increase the complexity of surgery for choledochal cysts (CDC). The laparoscopic approach for the management of paediatric CDCs with variant anatomy is underreported. This study aimed to describe anatomical variations, operative techniques and early outcomes of laparoscopic hepaticojejunostomy (HJ) in children with CDCs and variant anatomy.</p><p><strong>Patients and methods: </strong>We conducted a retrospective review of 40 children who underwent laparoscopic CDC excision with HJ between 2019 and 2024 in a single surgical unit. Patients were divided into Group I (with anatomical variations, n = 20) and Group II (without variations, n = 20). Data on demographic details, clinical presentation, imaging findings, pre-operative interventions, ductal and vascular anatomical variations, surgical techniques, intraoperative variables, post-operative complications and outcomes were collected and analysed.</p><p><strong>Results: </strong>Ductal variations were found in 10 patients, with aberrant right posterior sectoral duct being the most common. Vascular variations were identified in 12 patients, with anteriorly crossing the right hepatic artery (RHA) being the most frequent. Group I had a higher mean age (7.32 vs. 3.57 years, P = 0.014) and longer operative times (415 vs. 364 min, P < 0.0001). Conversion to laparotomy was necessary in 10% of Group I and 15% of Group II patients ( P = 0.634). Post-operative complications, primarily minor (Clavien-Dindo Grade I or II), occurred in 40% of Group I and 30% of Group II ( P = 0.495). Group I had a significantly shorter time to full feeds (72 vs. 80 h, P = 0.015). Both groups had similar post-operative hospital stays and follow-up durations. At the last follow-up, all patients, except one with liver failure in Group II, were asymptomatic with no significant biliary dilatation or liver function abnormalities.</p><p><strong>Conclusion: </strong>Laparoscopic management of CDCs with variant ductal and vascular anatomy in children is feasible, safe and effective. Detailed pre-operative imaging, meticulous intraoperative assessment and tailored surgical techniques are crucial for successful outcomes.</p>\",\"PeriodicalId\":48905,\"journal\":{\"name\":\"Journal of Minimal Access Surgery\",\"volume\":\" \",\"pages\":\"282-291\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12327796/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Minimal Access Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/jmas.jmas_255_24\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Minimal Access Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/jmas.jmas_255_24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
导言:胆管和肝血管解剖结构的变化增加了胆总管囊肿手术的复杂性。腹腔镜方法的管理儿科疾病控制与变异解剖是少报道。本研究旨在描述患有cdc和不同解剖结构的儿童腹腔镜肝空肠吻合术(HJ)的解剖变异、手术技术和早期结果。患者和方法:我们对40名在2019年至2024年期间在单个手术单元接受腹腔镜CDC切除HJ的儿童进行了回顾性研究。患者分为ⅰ组(有解剖变异,n = 20)和ⅱ组(无解剖变异,n = 20)。收集和分析人口统计学细节、临床表现、影像学表现、术前干预、导管和血管解剖变异、手术技术、术中变量、术后并发症和结果的数据。结果:10例患者均出现导管变异,以右侧后部门导管异常最为常见。在12例患者中发现血管变异,以右肝动脉(RHA)前交叉最为常见。I组患者平均年龄较高(7.32 vs. 3.57岁,P = 0.014),手术时间较长(415 vs. 364 min, P < 0.0001)。10%的I组患者和15%的II组患者需要转为剖腹手术(P = 0.634)。术后并发症主要为轻微(Clavien-Dindo I级或II级),I组40%,II组30% (P = 0.495)。第1组至完全饲喂所需时间显著缩短(72 h vs. 80 h, P = 0.015)。两组术后住院时间和随访时间相似。在最后一次随访时,除II组1例肝功能衰竭外,所有患者均无症状,无明显胆道扩张或肝功能异常。结论:腹腔镜下治疗儿童导管及血管解剖结构变异的疾病是可行、安全、有效的。详细的术前影像,细致的术中评估和量身定制的手术技术是成功的关键。
Laparoscopic management of variant ductal and vascular anatomy in children with choledochal cysts.
Introduction: Variations in biliary ductal and hepatic vascular anatomy increase the complexity of surgery for choledochal cysts (CDC). The laparoscopic approach for the management of paediatric CDCs with variant anatomy is underreported. This study aimed to describe anatomical variations, operative techniques and early outcomes of laparoscopic hepaticojejunostomy (HJ) in children with CDCs and variant anatomy.
Patients and methods: We conducted a retrospective review of 40 children who underwent laparoscopic CDC excision with HJ between 2019 and 2024 in a single surgical unit. Patients were divided into Group I (with anatomical variations, n = 20) and Group II (without variations, n = 20). Data on demographic details, clinical presentation, imaging findings, pre-operative interventions, ductal and vascular anatomical variations, surgical techniques, intraoperative variables, post-operative complications and outcomes were collected and analysed.
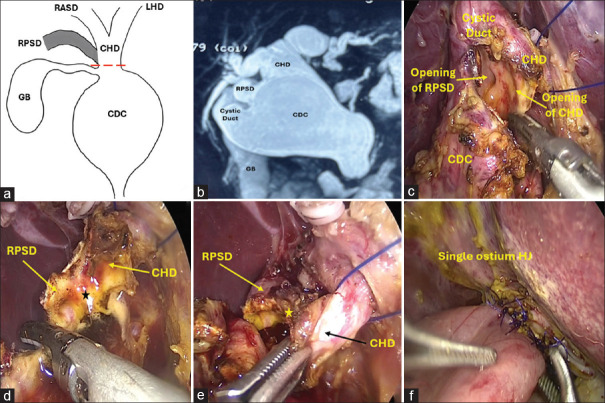
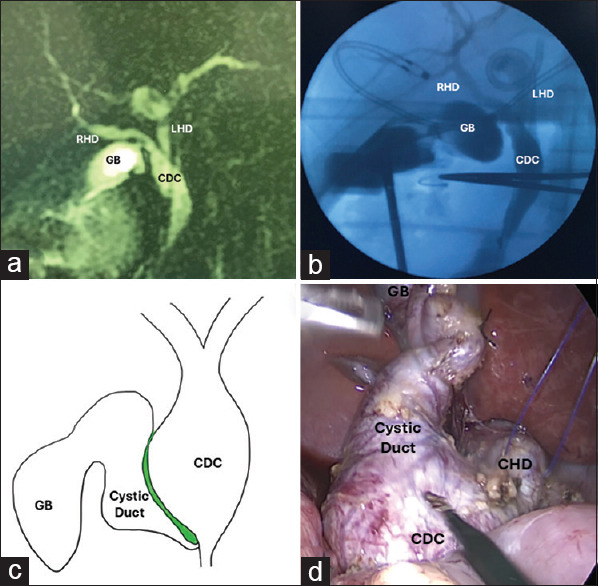
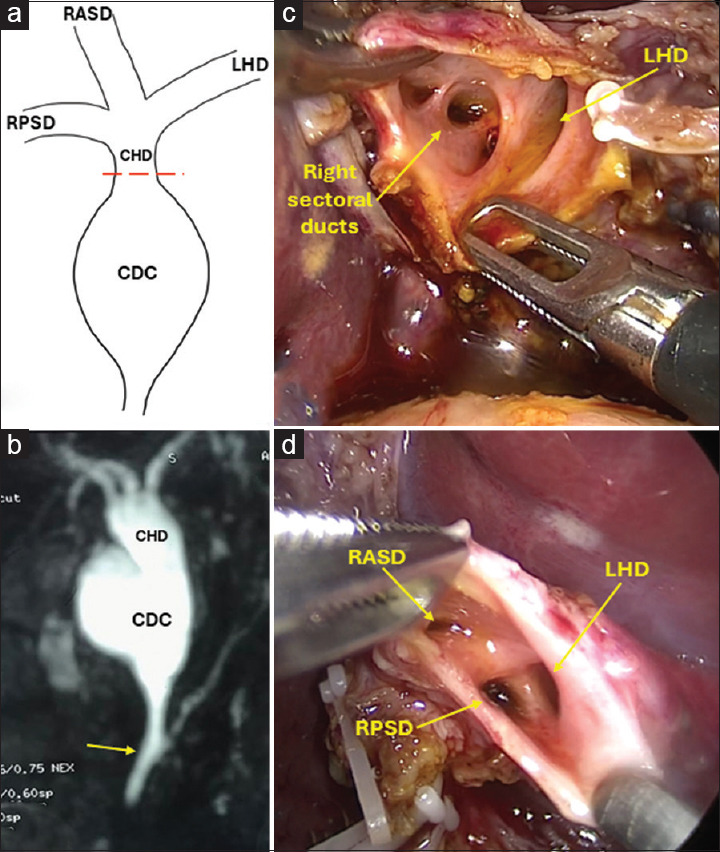
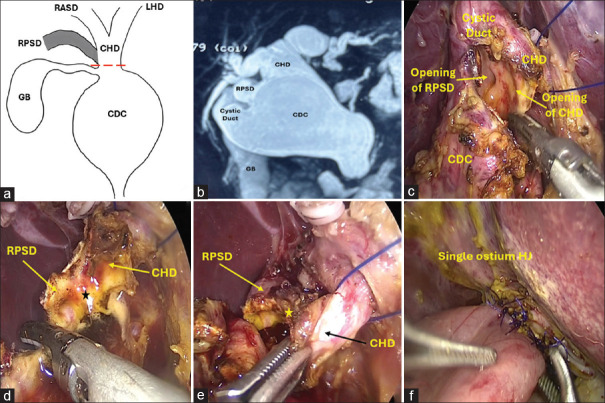
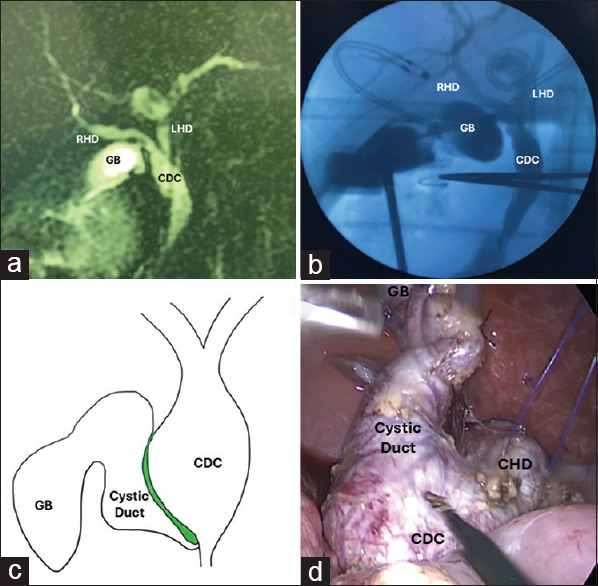
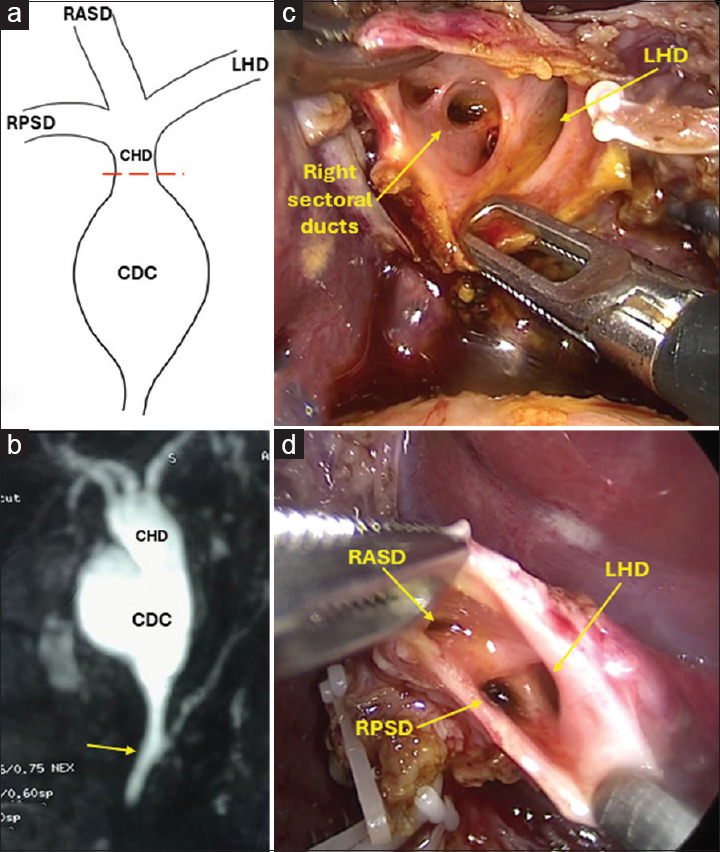
Results: Ductal variations were found in 10 patients, with aberrant right posterior sectoral duct being the most common. Vascular variations were identified in 12 patients, with anteriorly crossing the right hepatic artery (RHA) being the most frequent. Group I had a higher mean age (7.32 vs. 3.57 years, P = 0.014) and longer operative times (415 vs. 364 min, P < 0.0001). Conversion to laparotomy was necessary in 10% of Group I and 15% of Group II patients ( P = 0.634). Post-operative complications, primarily minor (Clavien-Dindo Grade I or II), occurred in 40% of Group I and 30% of Group II ( P = 0.495). Group I had a significantly shorter time to full feeds (72 vs. 80 h, P = 0.015). Both groups had similar post-operative hospital stays and follow-up durations. At the last follow-up, all patients, except one with liver failure in Group II, were asymptomatic with no significant biliary dilatation or liver function abnormalities.
Conclusion: Laparoscopic management of CDCs with variant ductal and vascular anatomy in children is feasible, safe and effective. Detailed pre-operative imaging, meticulous intraoperative assessment and tailored surgical techniques are crucial for successful outcomes.
期刊介绍:
Journal of Minimal Access Surgery (JMAS), the official publication of Indian Association of Gastrointestinal Endo Surgeons, launched in early 2005. The JMAS, a quarterly publication, is the first English-language journal from India, as also from this part of the world, dedicated to Minimal Access Surgery. The JMAS boasts an outstanding editorial board comprising of Indian and international experts in the field.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
