Sergio Velasco Malagón, Estivalis Acosta-Gutiérrez, José Atilio Nuñez Ramos, Sebastián Salinas, Guillermo Mora Pabón
{"title":"出院时通过护理点超声(POCUS)评估的亚临床充血可预测急性心力衰竭患者的再入院:预后队列研究","authors":"Sergio Velasco Malagón, Estivalis Acosta-Gutiérrez, José Atilio Nuñez Ramos, Sebastián Salinas, Guillermo Mora Pabón","doi":"10.24908/pocus.v9i2.17709","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Heart failure (HF) is a complex entity that increases the risk of adverse outcomes. Point of care ultrasound (POCUS) allows easy lung and systemic venous congestion identification. Using ultrasound to detect sub-clinical congestion at discharge may help predict readmissions and mortality. <b>Outcomes:</b> The primary outcome was to address 30-day rehospitalization, and as a secondary outcome we investigated readmission and mortality in patients with residual congestion assessed with POCUS. <b>Methods:</b> A prospective prognostic cohort study was conducted at a tertiary-level institution in Colombia. Patients with acute decompensated heart failure (ADHF) at discharge were evaluated using POCUS through lung ultrasound (LUS), portal vein pulsatility (PVP), and a composite assessment of residual congestion. Inclusion criteria were ADHF, over 18 years old, with a \"warm-wet\" clinical profile. POCUS was performed using an ultraportable device using LUS and PVP. Statistical analysis used logistic regression models to estimate the association between ultrasound congestion and outcomes. <b>Results:</b> A total of100 patients were included. The population was mostly female, with a median age of 78 years; 59% were hypertensive, and 39% had type 2 diabetes. Median NT-ProBNP was 3878 pg/ml. At discharge, 55% of patient had an inferior vena cava (IVC) over 2 cm, 54% had interstitial syndrome, and 41% had PVP >30%. Regarding 30-day readmission, we found an odds ratio (OR) 7.22 (95% CI 2.7-19.3) for interstitial syndrome; for PVP >30%, an OR 24.61 (95% CI 7.7-78.1) and an OR 13.19 (95% CI 2.7-62.6) for composite of residual congestion. <b>Conclusion:</b> Patients with ADHF and sub-clinical congestion, evidenced in LUS and PVP, were more likely to have readmission within 30 days of discharge. These findings should be confirmed with clinical trials to assess the effectiveness of a POCUS-guided treatment.</p>","PeriodicalId":74470,"journal":{"name":"POCUS journal","volume":"9 2","pages":"125-132"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11616985/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subclinical Congestion Evaluated by Point of Care Ultrasound (POCUS) at Discharge Predicts Readmission in Patients with Acute Heart Failure: Prognostic Cohort Study.\",\"authors\":\"Sergio Velasco Malagón, Estivalis Acosta-Gutiérrez, José Atilio Nuñez Ramos, Sebastián Salinas, Guillermo Mora Pabón\",\"doi\":\"10.24908/pocus.v9i2.17709\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Heart failure (HF) is a complex entity that increases the risk of adverse outcomes. Point of care ultrasound (POCUS) allows easy lung and systemic venous congestion identification. Using ultrasound to detect sub-clinical congestion at discharge may help predict readmissions and mortality. <b>Outcomes:</b> The primary outcome was to address 30-day rehospitalization, and as a secondary outcome we investigated readmission and mortality in patients with residual congestion assessed with POCUS. <b>Methods:</b> A prospective prognostic cohort study was conducted at a tertiary-level institution in Colombia. Patients with acute decompensated heart failure (ADHF) at discharge were evaluated using POCUS through lung ultrasound (LUS), portal vein pulsatility (PVP), and a composite assessment of residual congestion. Inclusion criteria were ADHF, over 18 years old, with a \\\"warm-wet\\\" clinical profile. POCUS was performed using an ultraportable device using LUS and PVP. Statistical analysis used logistic regression models to estimate the association between ultrasound congestion and outcomes. <b>Results:</b> A total of100 patients were included. The population was mostly female, with a median age of 78 years; 59% were hypertensive, and 39% had type 2 diabetes. Median NT-ProBNP was 3878 pg/ml. At discharge, 55% of patient had an inferior vena cava (IVC) over 2 cm, 54% had interstitial syndrome, and 41% had PVP >30%. Regarding 30-day readmission, we found an odds ratio (OR) 7.22 (95% CI 2.7-19.3) for interstitial syndrome; for PVP >30%, an OR 24.61 (95% CI 7.7-78.1) and an OR 13.19 (95% CI 2.7-62.6) for composite of residual congestion. <b>Conclusion:</b> Patients with ADHF and sub-clinical congestion, evidenced in LUS and PVP, were more likely to have readmission within 30 days of discharge. These findings should be confirmed with clinical trials to assess the effectiveness of a POCUS-guided treatment.</p>\",\"PeriodicalId\":74470,\"journal\":{\"name\":\"POCUS journal\",\"volume\":\"9 2\",\"pages\":\"125-132\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11616985/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"POCUS journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24908/pocus.v9i2.17709\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"POCUS journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24908/pocus.v9i2.17709","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
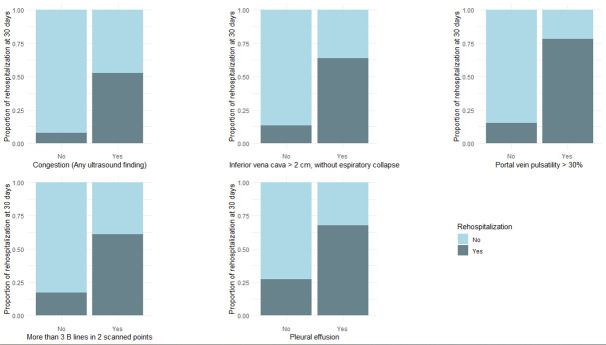
背景:心力衰竭(HF)是一个复杂的实体,增加了不良后果的风险。点护理超声(POCUS)可以很容易地识别肺部和全身静脉充血。使用超声检测出院时的亚临床充血可能有助于预测再入院率和死亡率。结果:主要结果是解决30天再住院问题,作为次要结果,我们调查了POCUS评估的残余充血患者的再入院和死亡率。方法:在哥伦比亚的一所三级机构进行前瞻性预后队列研究。急性失代偿性心力衰竭(ADHF)患者出院时采用POCUS通过肺超声(LUS)、门静脉搏动(PVP)和残余充血的综合评估进行评估。纳入标准为ADHF, 18岁以上,具有“温湿”临床特征。POCUS采用超便携设备,使用LUS和PVP。统计分析采用logistic回归模型估计超声充血与预后之间的关系。结果:共纳入100例患者。人口以女性为主,中位年龄为78岁;59%患有高血压,39%患有2型糖尿病。NT-ProBNP中位数为3878 pg/ml。出院时,55%的患者下腔静脉(IVC)超过2cm, 54%的患者有间质综合征,41%的患者有PVP, 30%的患者有PVP。关于30天再入院,我们发现间质综合征的比值比(OR)为7.22 (95% CI 2.7-19.3);对于PVP >30%, OR为24.61 (95% CI 7.7-78.1),剩余拥塞复合OR为13.19 (95% CI 2.7-62.6)。结论:以LUS和PVP为证据的ADHF和亚临床充血患者在出院后30天内再入院的可能性更大。这些发现应该通过临床试验来证实,以评估pocus引导治疗的有效性。
Subclinical Congestion Evaluated by Point of Care Ultrasound (POCUS) at Discharge Predicts Readmission in Patients with Acute Heart Failure: Prognostic Cohort Study.
Background: Heart failure (HF) is a complex entity that increases the risk of adverse outcomes. Point of care ultrasound (POCUS) allows easy lung and systemic venous congestion identification. Using ultrasound to detect sub-clinical congestion at discharge may help predict readmissions and mortality. Outcomes: The primary outcome was to address 30-day rehospitalization, and as a secondary outcome we investigated readmission and mortality in patients with residual congestion assessed with POCUS. Methods: A prospective prognostic cohort study was conducted at a tertiary-level institution in Colombia. Patients with acute decompensated heart failure (ADHF) at discharge were evaluated using POCUS through lung ultrasound (LUS), portal vein pulsatility (PVP), and a composite assessment of residual congestion. Inclusion criteria were ADHF, over 18 years old, with a "warm-wet" clinical profile. POCUS was performed using an ultraportable device using LUS and PVP. Statistical analysis used logistic regression models to estimate the association between ultrasound congestion and outcomes. Results: A total of100 patients were included. The population was mostly female, with a median age of 78 years; 59% were hypertensive, and 39% had type 2 diabetes. Median NT-ProBNP was 3878 pg/ml. At discharge, 55% of patient had an inferior vena cava (IVC) over 2 cm, 54% had interstitial syndrome, and 41% had PVP >30%. Regarding 30-day readmission, we found an odds ratio (OR) 7.22 (95% CI 2.7-19.3) for interstitial syndrome; for PVP >30%, an OR 24.61 (95% CI 7.7-78.1) and an OR 13.19 (95% CI 2.7-62.6) for composite of residual congestion. Conclusion: Patients with ADHF and sub-clinical congestion, evidenced in LUS and PVP, were more likely to have readmission within 30 days of discharge. These findings should be confirmed with clinical trials to assess the effectiveness of a POCUS-guided treatment.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
