{"title":"经肋显微内镜椎间盘切除术治疗中央胸椎间盘突出症引起的脊髓病:技术说明。","authors":"Masanari Takami, Kimihide Murakami, Kento Nonaka, Koji Hashimoto, Ryo Miyake, Hiroshi Yamada","doi":"10.22603/ssrr.2024-0097","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Minimally invasive surgical treatment of myelopathy caused by central thoracic disc herniation (TDH) is challenging to carry out because reaching the herniation site is difficult and the thoracic spinal cord is fragile. In this study, using the posterior-lateral approach for central TDH with myelopathy, we present a novel procedure of transcostal microendoscopic discectomy (TCMED).</p><p><strong>Technical note: </strong>The patient was operated in a prone position under general anesthesia. At a preoperatively determined distance from the midline, an 18-mm-long longitudinal incision was conducted, and using a 25-degree microendoscope, the operation was carried out. The endoscope was placed at an inward angle of approximately 50 degrees in the vertical direction. The ribs adjacent to the disc were identified, and the disc was exposed by resecting the ribs using a surgical high-speed drill while preserving the cortical bone of the ribs on the pleural side. The herniation was identified by drilling the ventral side of the disc and was then successfully removed. After discectomy, the dura mater expanded ventrally. Three male patients (mean age, 47.3 years) were treated, with 20 weeks of follow-up on average, 237.7-min mean operative time, and 26.7-mL mean blood loss. The average preoperative modified Japanese Orthopedic Association score was 5.2/11, which improved to 9.5/11 postoperatively, with a 75.6% average recovery rate. The 10-s step test score improved from an average of eight times preoperatively to 20 times postoperatively. No serious perioperative or postoperative complications or residual rib pain were observed.</p><p><strong>Conclusions: </strong>The proposed TCMED approach for treating central TDH that causes myelopathy allows for safe access to the level of the posterior vertebral wall using the rib as a landmark for resecting the rib head without opening the chest. Using the angled microendoscope and curved surgical instruments, the central TDH, located ventral to the spinal canal, can then be safely and effectively resected without spinal cord retraction.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"8 6","pages":"644-650"},"PeriodicalIF":1.2000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11625710/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transcostal Microendoscopic Discectomy for Central Thoracic Disc Herniation Causing Myelopathy: A Technical Note.\",\"authors\":\"Masanari Takami, Kimihide Murakami, Kento Nonaka, Koji Hashimoto, Ryo Miyake, Hiroshi Yamada\",\"doi\":\"10.22603/ssrr.2024-0097\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Minimally invasive surgical treatment of myelopathy caused by central thoracic disc herniation (TDH) is challenging to carry out because reaching the herniation site is difficult and the thoracic spinal cord is fragile. In this study, using the posterior-lateral approach for central TDH with myelopathy, we present a novel procedure of transcostal microendoscopic discectomy (TCMED).</p><p><strong>Technical note: </strong>The patient was operated in a prone position under general anesthesia. At a preoperatively determined distance from the midline, an 18-mm-long longitudinal incision was conducted, and using a 25-degree microendoscope, the operation was carried out. The endoscope was placed at an inward angle of approximately 50 degrees in the vertical direction. The ribs adjacent to the disc were identified, and the disc was exposed by resecting the ribs using a surgical high-speed drill while preserving the cortical bone of the ribs on the pleural side. The herniation was identified by drilling the ventral side of the disc and was then successfully removed. After discectomy, the dura mater expanded ventrally. Three male patients (mean age, 47.3 years) were treated, with 20 weeks of follow-up on average, 237.7-min mean operative time, and 26.7-mL mean blood loss. The average preoperative modified Japanese Orthopedic Association score was 5.2/11, which improved to 9.5/11 postoperatively, with a 75.6% average recovery rate. The 10-s step test score improved from an average of eight times preoperatively to 20 times postoperatively. No serious perioperative or postoperative complications or residual rib pain were observed.</p><p><strong>Conclusions: </strong>The proposed TCMED approach for treating central TDH that causes myelopathy allows for safe access to the level of the posterior vertebral wall using the rib as a landmark for resecting the rib head without opening the chest. Using the angled microendoscope and curved surgical instruments, the central TDH, located ventral to the spinal canal, can then be safely and effectively resected without spinal cord retraction.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"8 6\",\"pages\":\"644-650\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11625710/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2024-0097\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/27 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Transcostal Microendoscopic Discectomy for Central Thoracic Disc Herniation Causing Myelopathy: A Technical Note.
Introduction: Minimally invasive surgical treatment of myelopathy caused by central thoracic disc herniation (TDH) is challenging to carry out because reaching the herniation site is difficult and the thoracic spinal cord is fragile. In this study, using the posterior-lateral approach for central TDH with myelopathy, we present a novel procedure of transcostal microendoscopic discectomy (TCMED).
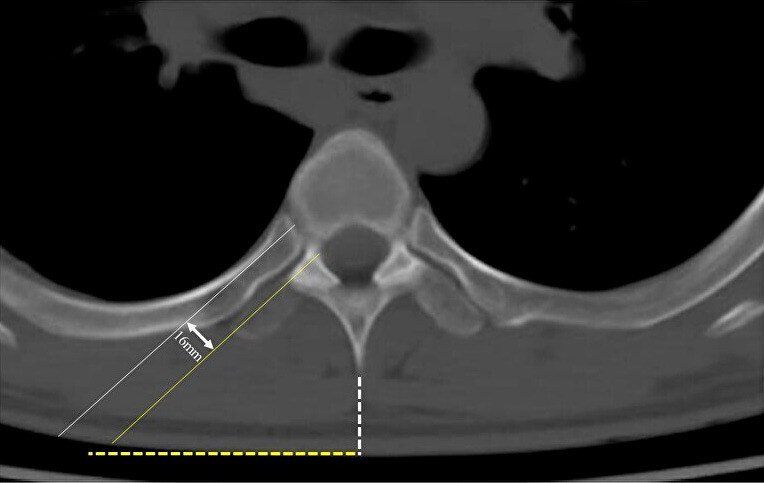
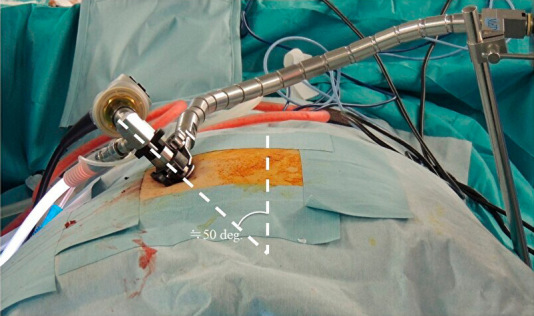
Technical note: The patient was operated in a prone position under general anesthesia. At a preoperatively determined distance from the midline, an 18-mm-long longitudinal incision was conducted, and using a 25-degree microendoscope, the operation was carried out. The endoscope was placed at an inward angle of approximately 50 degrees in the vertical direction. The ribs adjacent to the disc were identified, and the disc was exposed by resecting the ribs using a surgical high-speed drill while preserving the cortical bone of the ribs on the pleural side. The herniation was identified by drilling the ventral side of the disc and was then successfully removed. After discectomy, the dura mater expanded ventrally. Three male patients (mean age, 47.3 years) were treated, with 20 weeks of follow-up on average, 237.7-min mean operative time, and 26.7-mL mean blood loss. The average preoperative modified Japanese Orthopedic Association score was 5.2/11, which improved to 9.5/11 postoperatively, with a 75.6% average recovery rate. The 10-s step test score improved from an average of eight times preoperatively to 20 times postoperatively. No serious perioperative or postoperative complications or residual rib pain were observed.
Conclusions: The proposed TCMED approach for treating central TDH that causes myelopathy allows for safe access to the level of the posterior vertebral wall using the rib as a landmark for resecting the rib head without opening the chest. Using the angled microendoscope and curved surgical instruments, the central TDH, located ventral to the spinal canal, can then be safely and effectively resected without spinal cord retraction.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
