Yogesh Sharma, Campbell Thompson, Angelo Zinellu, Rashmi Shahi, Chris Horwood, Arduino A Mangoni
{"title":"中性粒细胞与淋巴细胞比率在预测社区获得性肺炎患者预后中的作用。","authors":"Yogesh Sharma, Campbell Thompson, Angelo Zinellu, Rashmi Shahi, Chris Horwood, Arduino A Mangoni","doi":"10.1016/j.clinme.2024.100278","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The value of the neutrophil-to-lymphocyte ratio (NLR) in predicting outcomes in patients hospitalised with community-acquired pneumonia (CAP) remains debated. This study evaluated whether NLR independently predicts clinical outcomes and enhances the predictive performance of the CURB-65 score in patients with CAP.</p><p><strong>Methods: </strong>Data from CAP admissions at two Australian hospitals from 2018 to 2023 were analysed. NLR was calculated using admission neutrophil and lymphocyte counts. Patients were categorised into NLR >12 and NLR ≤12. Multilevel-multivariable regression models, adjusting for age, sex, Charlson index, CURB-65 score, Hospital Frailty Risk Score (HFRS) and C-reactive protein (CRP), assessed outcomes including length of stay (LOS), intensive care unit (ICU) admission and in-hospital mortality.</p><p><strong>Results: </strong>Over 6 years, 7,862 patients with CAP were hospitalised (mean age 75.1 years, 54.6% male). Mean NLR was 12.6, with 2,877 (36.6%) patients having an NLR >12. Those with NLR >12 were older males with higher disease severity and Charlson index (p<0.05). Adjusted analyses showed that NLR >12 was independently associated with prolonged LOS (IRR=1.11, 95% CI 1.08-1.13, p<0.001), increased risk of ICU admission (adjusted odds ratio (aOR) =1.41, 95% confidence interval (CI) 1.06-1.88, p=0.019), and higher in-hospital mortality (aOR=1.27, 95% CI 1.06-1.53, p=0.009). The predictive ability of the CURB-65 score for in-hospital mortality was good (area under the curve (AUC) 0.68, 95% CI 0.66-0.70), while it was modest for the NLR (AUC 0.58, 95% CI 0.56-0.60). Incorporation of NLR to the CURB-65 score did not enhance its predictive ability (AUC 0.69, p>0.05).</p><p><strong>Conclusions: </strong>NLR independently predicts adverse outcomes in patients hospitalised with CAP but does not improve the predictive performance of the CURB-65 score.</p>","PeriodicalId":10492,"journal":{"name":"Clinical Medicine","volume":" ","pages":"100278"},"PeriodicalIF":3.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11731571/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of the neutrophil-to-lymphocyte ratio in predicting outcomes among patients with community-acquired pneumonia.\",\"authors\":\"Yogesh Sharma, Campbell Thompson, Angelo Zinellu, Rashmi Shahi, Chris Horwood, Arduino A Mangoni\",\"doi\":\"10.1016/j.clinme.2024.100278\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The value of the neutrophil-to-lymphocyte ratio (NLR) in predicting outcomes in patients hospitalised with community-acquired pneumonia (CAP) remains debated. This study evaluated whether NLR independently predicts clinical outcomes and enhances the predictive performance of the CURB-65 score in patients with CAP.</p><p><strong>Methods: </strong>Data from CAP admissions at two Australian hospitals from 2018 to 2023 were analysed. NLR was calculated using admission neutrophil and lymphocyte counts. Patients were categorised into NLR >12 and NLR ≤12. Multilevel-multivariable regression models, adjusting for age, sex, Charlson index, CURB-65 score, Hospital Frailty Risk Score (HFRS) and C-reactive protein (CRP), assessed outcomes including length of stay (LOS), intensive care unit (ICU) admission and in-hospital mortality.</p><p><strong>Results: </strong>Over 6 years, 7,862 patients with CAP were hospitalised (mean age 75.1 years, 54.6% male). Mean NLR was 12.6, with 2,877 (36.6%) patients having an NLR >12. Those with NLR >12 were older males with higher disease severity and Charlson index (p<0.05). Adjusted analyses showed that NLR >12 was independently associated with prolonged LOS (IRR=1.11, 95% CI 1.08-1.13, p<0.001), increased risk of ICU admission (adjusted odds ratio (aOR) =1.41, 95% confidence interval (CI) 1.06-1.88, p=0.019), and higher in-hospital mortality (aOR=1.27, 95% CI 1.06-1.53, p=0.009). The predictive ability of the CURB-65 score for in-hospital mortality was good (area under the curve (AUC) 0.68, 95% CI 0.66-0.70), while it was modest for the NLR (AUC 0.58, 95% CI 0.56-0.60). Incorporation of NLR to the CURB-65 score did not enhance its predictive ability (AUC 0.69, p>0.05).</p><p><strong>Conclusions: </strong>NLR independently predicts adverse outcomes in patients hospitalised with CAP but does not improve the predictive performance of the CURB-65 score.</p>\",\"PeriodicalId\":10492,\"journal\":{\"name\":\"Clinical Medicine\",\"volume\":\" \",\"pages\":\"100278\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11731571/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.clinme.2024.100278\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.clinme.2024.100278","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的:中性粒细胞与淋巴细胞比率(NLR)在预测社区获得性肺炎(CAP)住院患者预后方面的价值仍存在争议。本研究评估了NLR是否能独立预测CAP患者的临床结果,并增强了CURB-65评分的预测性能。方法:分析2018年至2023年澳大利亚两家医院CAP入院数据。NLR通过入院中性粒细胞和淋巴细胞计数计算。将患者分为NLR≤12和NLR≤12。多水平多变量回归模型,调整了年龄、性别、Charlson指数、CURB-65评分、医院虚弱风险评分(HFRS)和c反应蛋白(CRP),评估了包括住院时间(LOS)、重症监护病房(ICU)入院和住院死亡率在内的结果。结果:6年间,共有7862例CAP患者住院,平均年龄75.1岁,男性54.6%。平均NLR为12.6,2877例(36.6%)患者有NLR。NLR bb0 12为老年男性,疾病严重程度较高,Charlson指数(p12)与LOS延长独立相关(IRR=1.11, 95% CI 1.08-1.13, p0.05)。结论:NLR独立预测住院CAP患者的不良结局,但不能提高CURB-65评分的预测性能。
The role of the neutrophil-to-lymphocyte ratio in predicting outcomes among patients with community-acquired pneumonia.
Objectives: The value of the neutrophil-to-lymphocyte ratio (NLR) in predicting outcomes in patients hospitalised with community-acquired pneumonia (CAP) remains debated. This study evaluated whether NLR independently predicts clinical outcomes and enhances the predictive performance of the CURB-65 score in patients with CAP.
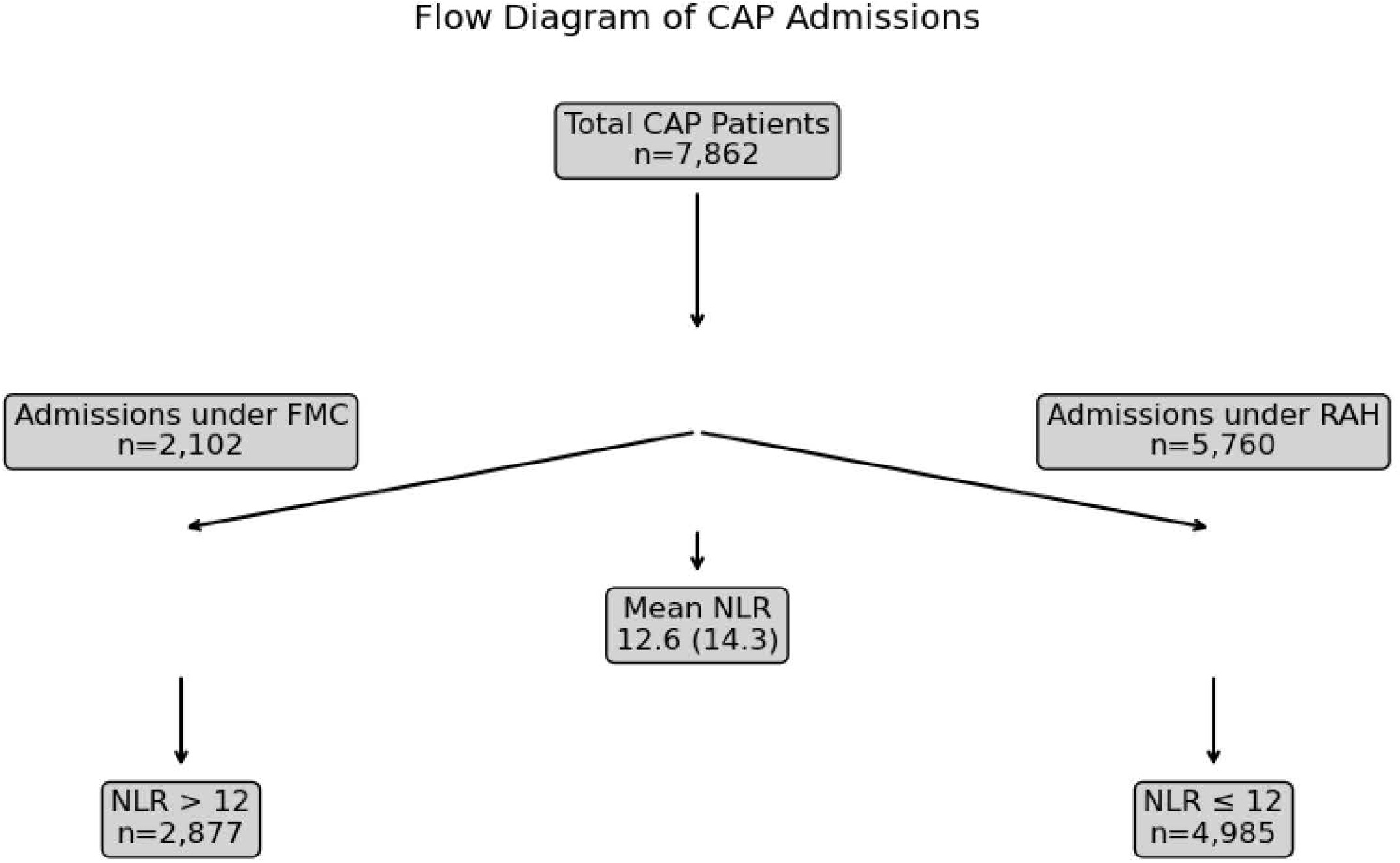
Methods: Data from CAP admissions at two Australian hospitals from 2018 to 2023 were analysed. NLR was calculated using admission neutrophil and lymphocyte counts. Patients were categorised into NLR >12 and NLR ≤12. Multilevel-multivariable regression models, adjusting for age, sex, Charlson index, CURB-65 score, Hospital Frailty Risk Score (HFRS) and C-reactive protein (CRP), assessed outcomes including length of stay (LOS), intensive care unit (ICU) admission and in-hospital mortality.
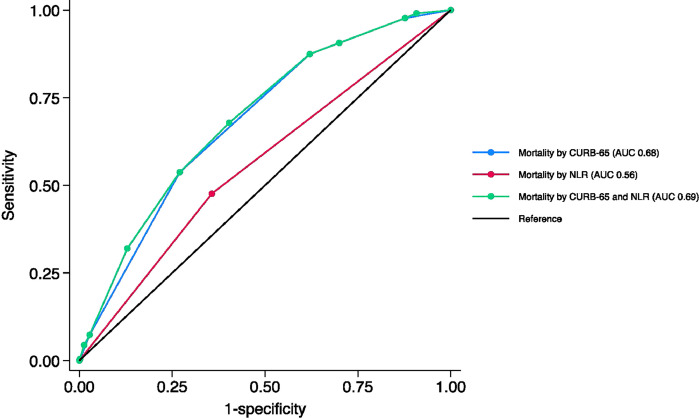
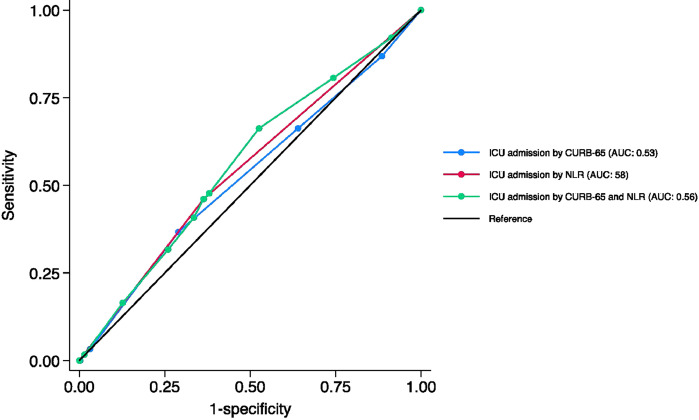
Results: Over 6 years, 7,862 patients with CAP were hospitalised (mean age 75.1 years, 54.6% male). Mean NLR was 12.6, with 2,877 (36.6%) patients having an NLR >12. Those with NLR >12 were older males with higher disease severity and Charlson index (p<0.05). Adjusted analyses showed that NLR >12 was independently associated with prolonged LOS (IRR=1.11, 95% CI 1.08-1.13, p<0.001), increased risk of ICU admission (adjusted odds ratio (aOR) =1.41, 95% confidence interval (CI) 1.06-1.88, p=0.019), and higher in-hospital mortality (aOR=1.27, 95% CI 1.06-1.53, p=0.009). The predictive ability of the CURB-65 score for in-hospital mortality was good (area under the curve (AUC) 0.68, 95% CI 0.66-0.70), while it was modest for the NLR (AUC 0.58, 95% CI 0.56-0.60). Incorporation of NLR to the CURB-65 score did not enhance its predictive ability (AUC 0.69, p>0.05).
Conclusions: NLR independently predicts adverse outcomes in patients hospitalised with CAP but does not improve the predictive performance of the CURB-65 score.
期刊介绍:
Clinical Medicine is aimed at practising physicians in the UK and overseas and has relevance to all those managing or working within the healthcare sector.
Available in print and online, the journal seeks to encourage high standards of medical care by promoting good clinical practice through original research, review and comment. The journal also includes a dedicated continuing medical education (CME) section in each issue. This presents the latest advances in a chosen specialty, with self-assessment questions at the end of each topic enabling CPD accreditation to be acquired.
ISSN: 1470-2118 E-ISSN: 1473-4893 Frequency: 6 issues per year




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
