Pardis Seyedi, Dionne Aleman, Nancy Baxter, Chaim Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott Emerson, Anna Gagliardi, Jonathan Irish, Danielle Martin, Samantha Lee, Marcy Saxe-Braithwaite, Julie Takata, Suting Yang, Claudia Zanchetta, David Urbach
{"title":"安大略省常见外科手术的转诊模式:一项横断面人群研究。","authors":"Pardis Seyedi, Dionne Aleman, Nancy Baxter, Chaim Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott Emerson, Anna Gagliardi, Jonathan Irish, Danielle Martin, Samantha Lee, Marcy Saxe-Braithwaite, Julie Takata, Suting Yang, Claudia Zanchetta, David Urbach","doi":"10.1503/cjs.002324","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Little is known about the existing structure and function of referral networks in the prevalent referral system for specialized surgical care in Canada, which is based on direct physician referral to specialists in a largely unmanaged referral marketplace. Our objective was to describe and analyze the referral networks of referring physicians and surgeons for common surgical procedures in Ontario, to better understand potential barriers to single-entry models.</p><p><strong>Methods: </strong>We analyzed referral networks for patients between referring physicians and surgeons for 9 common scheduled surgical procedures from 2016 to 2019 using administrative data sources in Ontario. We described the connectedness of referring physician-surgeon pairs using descriptive measures and graphical social network analysis.</p><p><strong>Results: </strong>The median number of surgeons connected to a referring physician for patients having a particular surgical procedure ranged from 1 (interquartile range [IQR] 1-3) for spine surgery to 3 (IQR 1-4) for knee arthroplasty and 3 (IQR 2-5) for noncancer uterine procedures. Referral network structure varied according to the procedure studied. Spine surgery was highly clustered with a small number of larger groups; gallbladder, inguinal hernia, and noncancer uterine surgery were highly distributed with many small groups within the referral network. Breast cancer surgery occurred in a largely distributed network, but with a skewed distribution reflecting a few small groups with large numbers of patients.</p><p><strong>Conclusion: </strong>Improving surgical wait times by coordinating surgical referrals will require approaches that address the structure of existing referral networks. Most physicians refer their patients to a very small number of surgeons, suggesting that referring physicians largely do not individualize referrals to multiple different surgeons based on specific patient characteristics.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"67 6","pages":"E397-E405"},"PeriodicalIF":2.2000,"publicationDate":"2024-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11649187/pdf/","citationCount":"0","resultStr":"{\"title\":\"Referral patterns for common surgical procedures in Ontario: a cross-sectional population-level study.\",\"authors\":\"Pardis Seyedi, Dionne Aleman, Nancy Baxter, Chaim Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott Emerson, Anna Gagliardi, Jonathan Irish, Danielle Martin, Samantha Lee, Marcy Saxe-Braithwaite, Julie Takata, Suting Yang, Claudia Zanchetta, David Urbach\",\"doi\":\"10.1503/cjs.002324\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Little is known about the existing structure and function of referral networks in the prevalent referral system for specialized surgical care in Canada, which is based on direct physician referral to specialists in a largely unmanaged referral marketplace. Our objective was to describe and analyze the referral networks of referring physicians and surgeons for common surgical procedures in Ontario, to better understand potential barriers to single-entry models.</p><p><strong>Methods: </strong>We analyzed referral networks for patients between referring physicians and surgeons for 9 common scheduled surgical procedures from 2016 to 2019 using administrative data sources in Ontario. We described the connectedness of referring physician-surgeon pairs using descriptive measures and graphical social network analysis.</p><p><strong>Results: </strong>The median number of surgeons connected to a referring physician for patients having a particular surgical procedure ranged from 1 (interquartile range [IQR] 1-3) for spine surgery to 3 (IQR 1-4) for knee arthroplasty and 3 (IQR 2-5) for noncancer uterine procedures. Referral network structure varied according to the procedure studied. Spine surgery was highly clustered with a small number of larger groups; gallbladder, inguinal hernia, and noncancer uterine surgery were highly distributed with many small groups within the referral network. Breast cancer surgery occurred in a largely distributed network, but with a skewed distribution reflecting a few small groups with large numbers of patients.</p><p><strong>Conclusion: </strong>Improving surgical wait times by coordinating surgical referrals will require approaches that address the structure of existing referral networks. Most physicians refer their patients to a very small number of surgeons, suggesting that referring physicians largely do not individualize referrals to multiple different surgeons based on specific patient characteristics.</p>\",\"PeriodicalId\":9573,\"journal\":{\"name\":\"Canadian Journal of Surgery\",\"volume\":\"67 6\",\"pages\":\"E397-E405\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-12-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11649187/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1503/cjs.002324\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.002324","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Referral patterns for common surgical procedures in Ontario: a cross-sectional population-level study.
Background: Little is known about the existing structure and function of referral networks in the prevalent referral system for specialized surgical care in Canada, which is based on direct physician referral to specialists in a largely unmanaged referral marketplace. Our objective was to describe and analyze the referral networks of referring physicians and surgeons for common surgical procedures in Ontario, to better understand potential barriers to single-entry models.
Methods: We analyzed referral networks for patients between referring physicians and surgeons for 9 common scheduled surgical procedures from 2016 to 2019 using administrative data sources in Ontario. We described the connectedness of referring physician-surgeon pairs using descriptive measures and graphical social network analysis.
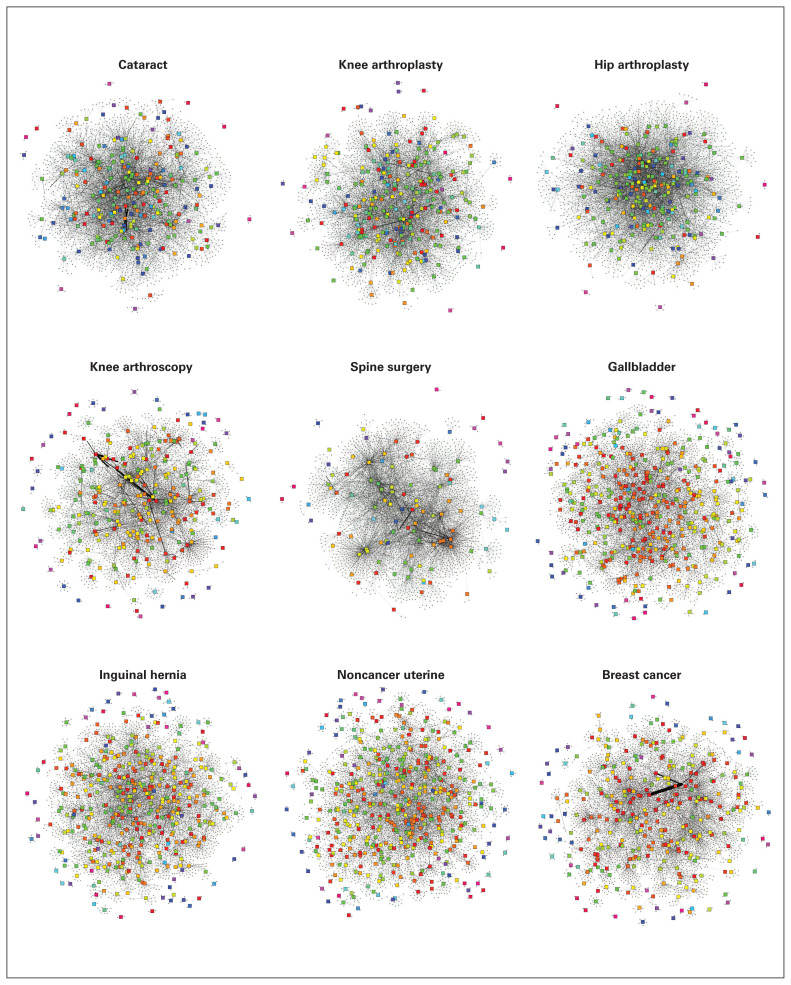
Results: The median number of surgeons connected to a referring physician for patients having a particular surgical procedure ranged from 1 (interquartile range [IQR] 1-3) for spine surgery to 3 (IQR 1-4) for knee arthroplasty and 3 (IQR 2-5) for noncancer uterine procedures. Referral network structure varied according to the procedure studied. Spine surgery was highly clustered with a small number of larger groups; gallbladder, inguinal hernia, and noncancer uterine surgery were highly distributed with many small groups within the referral network. Breast cancer surgery occurred in a largely distributed network, but with a skewed distribution reflecting a few small groups with large numbers of patients.
Conclusion: Improving surgical wait times by coordinating surgical referrals will require approaches that address the structure of existing referral networks. Most physicians refer their patients to a very small number of surgeons, suggesting that referring physicians largely do not individualize referrals to multiple different surgeons based on specific patient characteristics.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
