{"title":"大脑基底节巨大新腔隙畸形的手术切除:病例报告。","authors":"Kunio Yokoyama, Naokado Ikeda, Yutaka Ito, Hidekazu Tanaka, Akira Sugie, Makoto Yamada, Masahiko Wanibuchi, Masahiro Kawanishi","doi":"10.2176/jns-nmc.2024-0190","DOIUrl":null,"url":null,"abstract":"<p><p>A 74-year-old woman had a lacunar infarction in the brainstem and was admitted to Takeda General Hospital for treatment. She had significant sequelae and was discharged with a Modified Rankin Scale 0. Imaging follow-up was conducted every year after discharge on an outpatient basis. Seven years later, MRI of the head revealed a previous cerebral hemorrhage in the right basal ganglia. The imaging findings reveal that the patient was diagnosed with cerebral hemorrhage due to a cavernous malformation. The patient was asymptomatic, so imaging follow-up was continued, but the cavernous malformation grew in size over the next 8 years and caused three more hemorrhages. The last hemorrhage caused damage to the right extrapyramidal tract, which resulted in rapid cognitive decline and tremors of the left upper limb. To remove the cavernous malformation, a transsylvian-anterior transinsular approach was employed. Involuntary movements of the left upper limb disappeared postoperatively. A de novo cavernous malformation rarely grows to such a large size as it did in this case. A cavernous malformation in the basal ganglia must be carefully removed, ensuring that the perforating branches of the middle cerebral artery, which includes the lenticulostriate arteries, that may run along the borders of the mass are not damaged.</p>","PeriodicalId":101331,"journal":{"name":"NMC case report journal","volume":"11 ","pages":"353-356"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11646680/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Resection of a Giant De Novo Cavernous Malformation in the Cerebral Basal Ganglia: Case Report.\",\"authors\":\"Kunio Yokoyama, Naokado Ikeda, Yutaka Ito, Hidekazu Tanaka, Akira Sugie, Makoto Yamada, Masahiko Wanibuchi, Masahiro Kawanishi\",\"doi\":\"10.2176/jns-nmc.2024-0190\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 74-year-old woman had a lacunar infarction in the brainstem and was admitted to Takeda General Hospital for treatment. She had significant sequelae and was discharged with a Modified Rankin Scale 0. Imaging follow-up was conducted every year after discharge on an outpatient basis. Seven years later, MRI of the head revealed a previous cerebral hemorrhage in the right basal ganglia. The imaging findings reveal that the patient was diagnosed with cerebral hemorrhage due to a cavernous malformation. The patient was asymptomatic, so imaging follow-up was continued, but the cavernous malformation grew in size over the next 8 years and caused three more hemorrhages. The last hemorrhage caused damage to the right extrapyramidal tract, which resulted in rapid cognitive decline and tremors of the left upper limb. To remove the cavernous malformation, a transsylvian-anterior transinsular approach was employed. Involuntary movements of the left upper limb disappeared postoperatively. A de novo cavernous malformation rarely grows to such a large size as it did in this case. A cavernous malformation in the basal ganglia must be carefully removed, ensuring that the perforating branches of the middle cerebral artery, which includes the lenticulostriate arteries, that may run along the borders of the mass are not damaged.</p>\",\"PeriodicalId\":101331,\"journal\":{\"name\":\"NMC case report journal\",\"volume\":\"11 \",\"pages\":\"353-356\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11646680/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC case report journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2024-0190\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC case report journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2024-0190","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Surgical Resection of a Giant De Novo Cavernous Malformation in the Cerebral Basal Ganglia: Case Report.
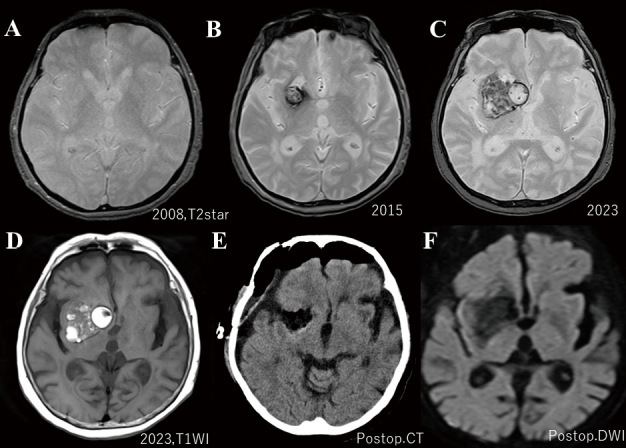
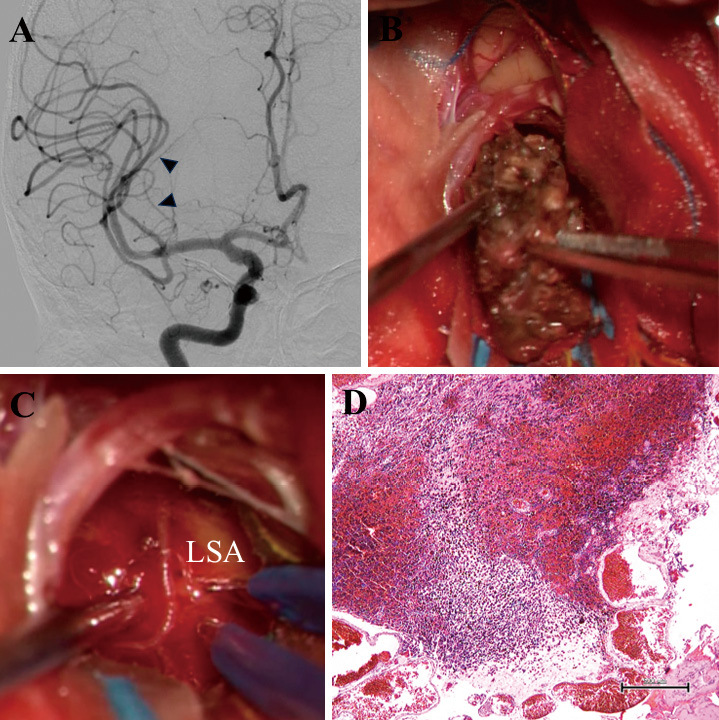
A 74-year-old woman had a lacunar infarction in the brainstem and was admitted to Takeda General Hospital for treatment. She had significant sequelae and was discharged with a Modified Rankin Scale 0. Imaging follow-up was conducted every year after discharge on an outpatient basis. Seven years later, MRI of the head revealed a previous cerebral hemorrhage in the right basal ganglia. The imaging findings reveal that the patient was diagnosed with cerebral hemorrhage due to a cavernous malformation. The patient was asymptomatic, so imaging follow-up was continued, but the cavernous malformation grew in size over the next 8 years and caused three more hemorrhages. The last hemorrhage caused damage to the right extrapyramidal tract, which resulted in rapid cognitive decline and tremors of the left upper limb. To remove the cavernous malformation, a transsylvian-anterior transinsular approach was employed. Involuntary movements of the left upper limb disappeared postoperatively. A de novo cavernous malformation rarely grows to such a large size as it did in this case. A cavernous malformation in the basal ganglia must be carefully removed, ensuring that the perforating branches of the middle cerebral artery, which includes the lenticulostriate arteries, that may run along the borders of the mass are not damaged.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
