Haibei Liu, Rong Luo, Liu Qian, Yujun Zhang, Wensheng Zhang, Juan Tan, Ling Ye
{"title":"右美托咪定对选择性腹部大手术后急性肾损伤的影响:一项回顾性单中心倾向评分匹配研究。","authors":"Haibei Liu, Rong Luo, Liu Qian, Yujun Zhang, Wensheng Zhang, Juan Tan, Ling Ye","doi":"10.1186/s12871-024-02845-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Major abdominal surgery is a kind of high-risk surgery type for postoperative acute kidney injury (AKI) among non-cardiac surgeries. Despite dexmedetomidine exerts significant renal protective effects in cardiac surgeries and animal studies, whether it is associated with a lower incidence of AKI in major abdominal surgeries remains unclear.</p><p><strong>Methods: </strong>From January 2019 to July 2021, patients undergoing elective major abdominal surgery in West China Hospital were enrolled. Participants were divided into two groups based on exposure to continuous intravenous dexmedetomidine: the Dex group (exposed) and the Control group (not exposed). The primary outcome was the incidence of AKI in the postoperative 7 days. Secondary outcomes included intraopertive average urine output, renal function on the first day after surgery, incidence of postoperative dialysis, postoperative intensive care unit (ICU) admission, in-hospital mortality, length of hospital stay, incidence of intraoperative hypotension and bradycardia, and intraoperative use of inotropes and vasopressors. Propensity score matching (PSM), based on participants' baseline and intraoperative characteristics, was performed to minimize potential bias. Furthermore, a subgroup analysis was conducted based on the infusion rate and the use of a loading dose to explore the effects of different methods of dexmedetomidine administration on AKI. The subgroups included: loading dose, non-loading dose, low-infusion rate (infusion rate ≤ 0.4 µg/kg/h), and high-infusion rate (infusion rate > 0.4 µg/kg/h).</p><p><strong>Results: </strong>After PSM with a ratio of 1:1, a total of 8836 patients were successfully matched. Dexmedetomidine administration had no association with the incidence of postoperative AKI, serum creatinine (Scr) level on the first postoperative day, incidence of postoperative dialysis, postoperative ICU admission, in-hospital mortality, length of hospital stay, intraoperative hypotension, or the use of inotropes and vasopressors, but had association with increased intraoperative average urine output (122.95 (76.80, 189.27) vs. 104.65 (67.04, 161.07) ml/h, P < 0.001), higher value of estimated glomerular filtration rate (eGFR) (97.33 ± 15.95 vs. 96.13 ± 16.35 ml/min/1.73m<sup>2</sup>, P < 0.001) on the first day after surgery and a higher incidence of intraoperative bradycardia (37.0% vs. 30.6%; P < 0.001). In the loading dose subgroup, dexmedetomidine use was significantly associated with a reduced incidence of postoperative AKI (odds ratio (OR): 0.44, 95% confidence interval (CI): 0.23-0.76, P = 0.006).The association between dexmedetomidine and postoperative AKI was absent in subgroups of high or low infusion rate and no loading dose use.</p><p><strong>Conclusion: </strong>In this single-center retrospective propensity-matched study, we did not detect a significant overall difference in post-operative AKI rates between patients treated with or without dexmedetomidine during major abdominal surgery. However, though additional prospective data are needed, our study found that administering dexmedetomidine with a loading dose may be associated with lower rates of AKI, potentially indicating a renoprotective effect of loading-dose dexmedetomidine in this setting.</p>","PeriodicalId":9190,"journal":{"name":"BMC Anesthesiology","volume":"24 1","pages":"456"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11657137/pdf/","citationCount":"0","resultStr":"{\"title\":\"The effect of dexmedetomidine on acute kidney injury after elective major abdominal surgery : a retrospective single-center propensity score matched study.\",\"authors\":\"Haibei Liu, Rong Luo, Liu Qian, Yujun Zhang, Wensheng Zhang, Juan Tan, Ling Ye\",\"doi\":\"10.1186/s12871-024-02845-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Major abdominal surgery is a kind of high-risk surgery type for postoperative acute kidney injury (AKI) among non-cardiac surgeries. Despite dexmedetomidine exerts significant renal protective effects in cardiac surgeries and animal studies, whether it is associated with a lower incidence of AKI in major abdominal surgeries remains unclear.</p><p><strong>Methods: </strong>From January 2019 to July 2021, patients undergoing elective major abdominal surgery in West China Hospital were enrolled. Participants were divided into two groups based on exposure to continuous intravenous dexmedetomidine: the Dex group (exposed) and the Control group (not exposed). The primary outcome was the incidence of AKI in the postoperative 7 days. Secondary outcomes included intraopertive average urine output, renal function on the first day after surgery, incidence of postoperative dialysis, postoperative intensive care unit (ICU) admission, in-hospital mortality, length of hospital stay, incidence of intraoperative hypotension and bradycardia, and intraoperative use of inotropes and vasopressors. Propensity score matching (PSM), based on participants' baseline and intraoperative characteristics, was performed to minimize potential bias. Furthermore, a subgroup analysis was conducted based on the infusion rate and the use of a loading dose to explore the effects of different methods of dexmedetomidine administration on AKI. The subgroups included: loading dose, non-loading dose, low-infusion rate (infusion rate ≤ 0.4 µg/kg/h), and high-infusion rate (infusion rate > 0.4 µg/kg/h).</p><p><strong>Results: </strong>After PSM with a ratio of 1:1, a total of 8836 patients were successfully matched. Dexmedetomidine administration had no association with the incidence of postoperative AKI, serum creatinine (Scr) level on the first postoperative day, incidence of postoperative dialysis, postoperative ICU admission, in-hospital mortality, length of hospital stay, intraoperative hypotension, or the use of inotropes and vasopressors, but had association with increased intraoperative average urine output (122.95 (76.80, 189.27) vs. 104.65 (67.04, 161.07) ml/h, P < 0.001), higher value of estimated glomerular filtration rate (eGFR) (97.33 ± 15.95 vs. 96.13 ± 16.35 ml/min/1.73m<sup>2</sup>, P < 0.001) on the first day after surgery and a higher incidence of intraoperative bradycardia (37.0% vs. 30.6%; P < 0.001). In the loading dose subgroup, dexmedetomidine use was significantly associated with a reduced incidence of postoperative AKI (odds ratio (OR): 0.44, 95% confidence interval (CI): 0.23-0.76, P = 0.006).The association between dexmedetomidine and postoperative AKI was absent in subgroups of high or low infusion rate and no loading dose use.</p><p><strong>Conclusion: </strong>In this single-center retrospective propensity-matched study, we did not detect a significant overall difference in post-operative AKI rates between patients treated with or without dexmedetomidine during major abdominal surgery. However, though additional prospective data are needed, our study found that administering dexmedetomidine with a loading dose may be associated with lower rates of AKI, potentially indicating a renoprotective effect of loading-dose dexmedetomidine in this setting.</p>\",\"PeriodicalId\":9190,\"journal\":{\"name\":\"BMC Anesthesiology\",\"volume\":\"24 1\",\"pages\":\"456\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-12-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11657137/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Anesthesiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12871-024-02845-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12871-024-02845-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:在非心脏手术中,腹部大手术是术后急性肾损伤(AKI)的高危手术类型。尽管右美托咪定在心脏手术和动物实验中具有显著的肾脏保护作用,但它是否与腹部大手术中AKI发生率较低有关尚不清楚。方法:选取2019年1月至2021年7月华西医院择期腹部大手术患者为研究对象。参与者根据持续静脉注射右美托咪定的暴露情况分为两组:右美托咪定组(暴露组)和对照组(未暴露组)。主要观察指标是术后7天内AKI的发生率。次要结局包括术中平均尿量、术后第一天肾功能、术后透析发生率、术后重症监护病房(ICU)入院率、住院死亡率、住院时间、术中低血压和心动过缓发生率、术中肌力药物和血管加压药物的使用。根据参与者的基线和术中特征进行倾向评分匹配(PSM),以尽量减少潜在的偏倚。此外,基于输注速率和负荷剂量进行亚组分析,探讨右美托咪定不同给药方式对AKI的影响。亚组分为:加载剂量组、非加载剂量组、低注射速率组(注射速率≤0.4µg/kg/h)、高注射速率组(注射速率> 0.4µg/kg/h)。结果:经1:1比例PSM后,成功匹配8836例患者。右美托咪定给药与术后AKI发生率、术后第1天血清肌酐(Scr)水平、术后透析发生率、术后ICU入院率、住院死亡率、住院时间、术中低血压、使用收缩性药物和升压药物无关,但与术中平均尿量增加(122.95(76.80,189.27)比104.65 (67.04,161.07)ml/h, P 2, P在这项单中心回顾性倾向匹配研究中,我们没有发现在腹部大手术中接受或不接受右美托咪定治疗的患者术后AKI发生率有显著的总体差异。然而,尽管需要额外的前瞻性数据,我们的研究发现,负荷剂量的右美托咪定可能与较低的AKI发生率相关,这可能表明负荷剂量的右美托咪定在这种情况下具有肾保护作用。
The effect of dexmedetomidine on acute kidney injury after elective major abdominal surgery : a retrospective single-center propensity score matched study.
Background: Major abdominal surgery is a kind of high-risk surgery type for postoperative acute kidney injury (AKI) among non-cardiac surgeries. Despite dexmedetomidine exerts significant renal protective effects in cardiac surgeries and animal studies, whether it is associated with a lower incidence of AKI in major abdominal surgeries remains unclear.
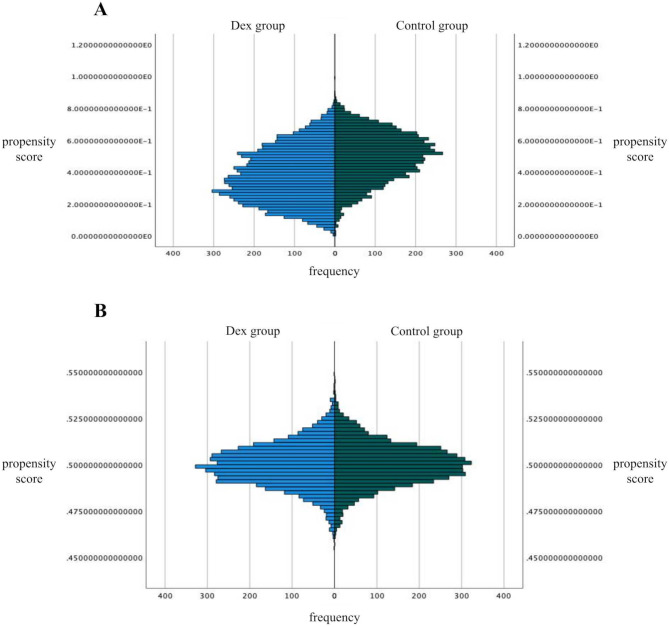
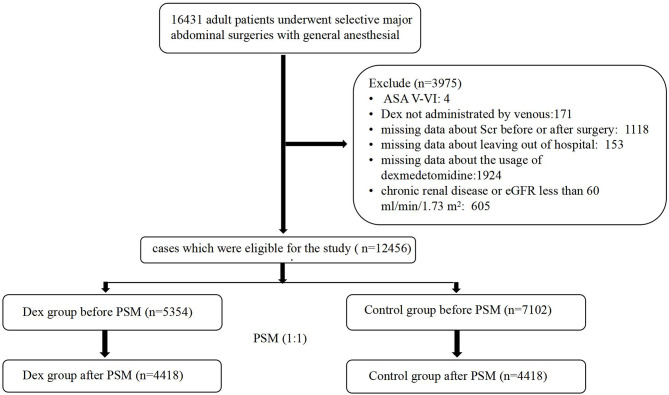
Methods: From January 2019 to July 2021, patients undergoing elective major abdominal surgery in West China Hospital were enrolled. Participants were divided into two groups based on exposure to continuous intravenous dexmedetomidine: the Dex group (exposed) and the Control group (not exposed). The primary outcome was the incidence of AKI in the postoperative 7 days. Secondary outcomes included intraopertive average urine output, renal function on the first day after surgery, incidence of postoperative dialysis, postoperative intensive care unit (ICU) admission, in-hospital mortality, length of hospital stay, incidence of intraoperative hypotension and bradycardia, and intraoperative use of inotropes and vasopressors. Propensity score matching (PSM), based on participants' baseline and intraoperative characteristics, was performed to minimize potential bias. Furthermore, a subgroup analysis was conducted based on the infusion rate and the use of a loading dose to explore the effects of different methods of dexmedetomidine administration on AKI. The subgroups included: loading dose, non-loading dose, low-infusion rate (infusion rate ≤ 0.4 µg/kg/h), and high-infusion rate (infusion rate > 0.4 µg/kg/h).
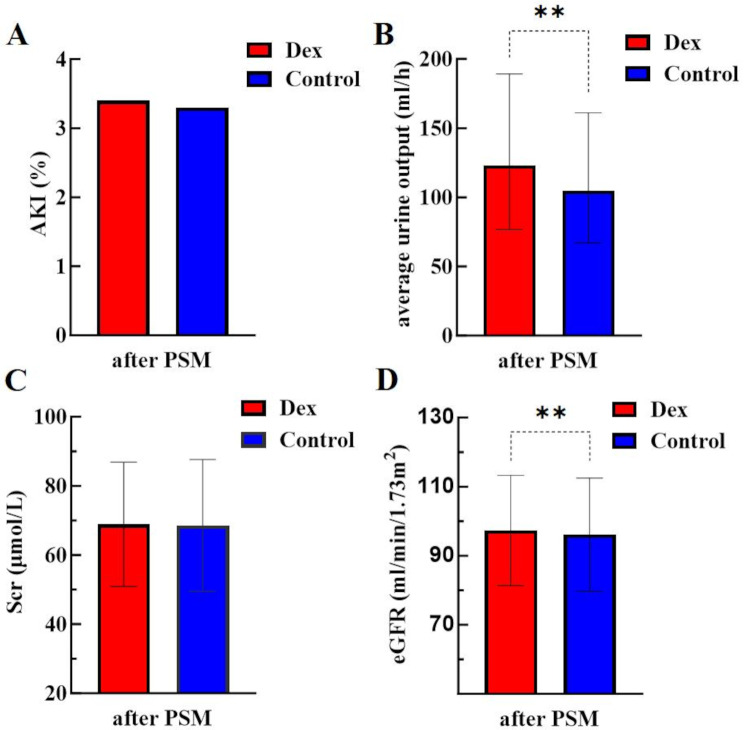
Results: After PSM with a ratio of 1:1, a total of 8836 patients were successfully matched. Dexmedetomidine administration had no association with the incidence of postoperative AKI, serum creatinine (Scr) level on the first postoperative day, incidence of postoperative dialysis, postoperative ICU admission, in-hospital mortality, length of hospital stay, intraoperative hypotension, or the use of inotropes and vasopressors, but had association with increased intraoperative average urine output (122.95 (76.80, 189.27) vs. 104.65 (67.04, 161.07) ml/h, P < 0.001), higher value of estimated glomerular filtration rate (eGFR) (97.33 ± 15.95 vs. 96.13 ± 16.35 ml/min/1.73m2, P < 0.001) on the first day after surgery and a higher incidence of intraoperative bradycardia (37.0% vs. 30.6%; P < 0.001). In the loading dose subgroup, dexmedetomidine use was significantly associated with a reduced incidence of postoperative AKI (odds ratio (OR): 0.44, 95% confidence interval (CI): 0.23-0.76, P = 0.006).The association between dexmedetomidine and postoperative AKI was absent in subgroups of high or low infusion rate and no loading dose use.
Conclusion: In this single-center retrospective propensity-matched study, we did not detect a significant overall difference in post-operative AKI rates between patients treated with or without dexmedetomidine during major abdominal surgery. However, though additional prospective data are needed, our study found that administering dexmedetomidine with a loading dose may be associated with lower rates of AKI, potentially indicating a renoprotective effect of loading-dose dexmedetomidine in this setting.
期刊介绍:
BMC Anesthesiology is an open access, peer-reviewed journal that considers articles on all aspects of anesthesiology, critical care, perioperative care and pain management, including clinical and experimental research into anesthetic mechanisms, administration and efficacy, technology and monitoring, and associated economic issues.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
