Alexandria Bennett, Nicole Shaver, Niyati Vyas, Faris Almoli, Robert Pap, Andrea Douglas, Taddele Kibret, Becky Skidmore, Martin Yaffe, Anna Wilkinson, Jean M Seely, Julian Little, David Moher
{"title":"乳腺癌筛查:为加拿大预防保健指南工作组提供的系统审查更新。","authors":"Alexandria Bennett, Nicole Shaver, Niyati Vyas, Faris Almoli, Robert Pap, Andrea Douglas, Taddele Kibret, Becky Skidmore, Martin Yaffe, Anna Wilkinson, Jean M Seely, Julian Little, David Moher","doi":"10.1186/s13643-024-02700-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This systematic review update synthesized recent evidence on the benefits and harms of breast cancer screening in women aged ≥ 40 years and aims to inform the Canadian Task Force on Preventive Health Care's (CTFPHC) guideline update.</p><p><strong>Methods: </strong>We searched Ovid MEDLINE® ALL, Embase Classic + Embase and Cochrane Central Register of Controlled Trials to update our searches to July 8, 2023. Search results for observational studies were limited to publication dates from 2014 to capture more relevant studies. Screening was performed independently and in duplicate by the review team. To expedite the screening process, machine learning was used to prioritize relevant references. Critical health outcomes, as outlined by the CTFPHC, included breast cancer and all-cause mortality, treatment-related morbidity and overdiagnosis. Randomized controlled trials (RCTs), non/quasi RCTs and observational studies were included. Data extraction and quality assessment were performed by one reviewer and verified by another. Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool for RCTs and the Joanna Brigg's Institute (JBI) checklists for non-randomized and observational studies. When deemed appropriate, studies were pooled via random-effects models. The overall certainty of the evidence was assessed following GRADE guidance.</p><p><strong>Results: </strong>Three new papers reporting on existing RCT trial data and 26 observational studies were included. No new RCTs were identified in this update. No study reported results by ethnicity, race, proportion of study population with dense breasts, or socioeconomic status. For breast cancer mortality, RCT data from the prior review reported a significant relative reduction in the risk of breast cancer mortality with screening mammography for a general population of 15% (RR 0.85 95% CI 0.78 to 0.93). In this review update, the breast cancer mortality relative risk reduction based on RCT data remained the same, and absolute effects by age decade over 10 years were 0.27 fewer deaths per 1000 in those aged 40 to 49; 0.50 fewer deaths per 1000 in those aged 50 to 59; 0.65 fewer deaths per 1000 in those aged 60 to 69; and 0.92 fewer deaths per 1000 in those aged 70 to 74. For observational data, the relative mortality risk reduction ranged from 29 to 62%. Absolute effects from breast cancer mortality over 10 years ranged from 0.79 to 0.94 fewer deaths per 1000 in those aged 40 to 49; 1.45 to 1.72 fewer deaths per 1000 in those aged 50 to 59; 1.89 to 2.24 fewer deaths per 1000 in those aged 60 to 69; and 2.68 to 3.17 fewer deaths per 1000 in those aged 70 to 74. For all-cause mortality, RCT data from the prior review reported a non-significant relative reduction in the risk of all-cause mortality of screening mammography for a general population of 1% (RR 0.99, 95% CI 0.98 to 1.00). In this review update, the absolute effects for all-cause mortality over 10 years by age decade were 0.13 fewer deaths per 1000 in those aged 40 to 49; 0.31 fewer deaths per 1000 in those aged 50 to 59; 0.71 fewer deaths per 1000 in those aged 60 to 69; and 1.41 fewer deaths per 1000 in those aged 70 to 74. No observational data were found for all-cause mortality. For overdiagnosis, this review update found the absolute effects for RCT data (range of follow-up between 9 and 15 years) to be 1.95 more invasive and in situ cancers per 1000, or 1 more invasive cancer per 1000, for those aged 40 to 49 and 1.93 more invasive and in situ cancers per 1000, or 1.18 more invasive cancers per 1000, for those aged 50 to 59. A sensitivity analysis removing high risk of bias studies found 1.57 more invasive and in situ cancers, or 0.49 more invasive cancers, per 1000 for those aged 40 to 49 and 3.95 more invasive and in situ cancers per 1000, or 2.81 more invasive cancers per 1000, in those aged 50 to 59. For observational data, one report (follow-up for 13 years) found 0.34 more invasive and in situ cancers per 1000 in those aged 50 to 69. Overall, the GRADE certainty of evidence was assessed as low or very low, suggesting that the evidence is very uncertain about the effect of screening for breast cancer on the outcomes evaluated in this review.</p><p><strong>Conclusions: </strong>This systematic review update did not identify any new trials comparing breast cancer screening to no screening. Although 26 new observational studies were identified, the overall quality of evidence remains generally low or very low. Future research initiatives should prioritize studying screening in higher risk populations such as those from different ages, racial or ethnic groups, with dense breasts or family history.</p><p><strong>Systematic review registration: </strong>Protocol available on the Open Science Framework: https://osf.io/xngsu/.</p>","PeriodicalId":22162,"journal":{"name":"Systematic Reviews","volume":"13 1","pages":"304"},"PeriodicalIF":3.9000,"publicationDate":"2024-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656969/pdf/","citationCount":"0","resultStr":"{\"title\":\"Screening for breast cancer: a systematic review update to inform the Canadian Task Force on Preventive Health Care guideline.\",\"authors\":\"Alexandria Bennett, Nicole Shaver, Niyati Vyas, Faris Almoli, Robert Pap, Andrea Douglas, Taddele Kibret, Becky Skidmore, Martin Yaffe, Anna Wilkinson, Jean M Seely, Julian Little, David Moher\",\"doi\":\"10.1186/s13643-024-02700-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This systematic review update synthesized recent evidence on the benefits and harms of breast cancer screening in women aged ≥ 40 years and aims to inform the Canadian Task Force on Preventive Health Care's (CTFPHC) guideline update.</p><p><strong>Methods: </strong>We searched Ovid MEDLINE® ALL, Embase Classic + Embase and Cochrane Central Register of Controlled Trials to update our searches to July 8, 2023. Search results for observational studies were limited to publication dates from 2014 to capture more relevant studies. Screening was performed independently and in duplicate by the review team. To expedite the screening process, machine learning was used to prioritize relevant references. Critical health outcomes, as outlined by the CTFPHC, included breast cancer and all-cause mortality, treatment-related morbidity and overdiagnosis. Randomized controlled trials (RCTs), non/quasi RCTs and observational studies were included. Data extraction and quality assessment were performed by one reviewer and verified by another. Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool for RCTs and the Joanna Brigg's Institute (JBI) checklists for non-randomized and observational studies. When deemed appropriate, studies were pooled via random-effects models. The overall certainty of the evidence was assessed following GRADE guidance.</p><p><strong>Results: </strong>Three new papers reporting on existing RCT trial data and 26 observational studies were included. No new RCTs were identified in this update. No study reported results by ethnicity, race, proportion of study population with dense breasts, or socioeconomic status. For breast cancer mortality, RCT data from the prior review reported a significant relative reduction in the risk of breast cancer mortality with screening mammography for a general population of 15% (RR 0.85 95% CI 0.78 to 0.93). In this review update, the breast cancer mortality relative risk reduction based on RCT data remained the same, and absolute effects by age decade over 10 years were 0.27 fewer deaths per 1000 in those aged 40 to 49; 0.50 fewer deaths per 1000 in those aged 50 to 59; 0.65 fewer deaths per 1000 in those aged 60 to 69; and 0.92 fewer deaths per 1000 in those aged 70 to 74. For observational data, the relative mortality risk reduction ranged from 29 to 62%. Absolute effects from breast cancer mortality over 10 years ranged from 0.79 to 0.94 fewer deaths per 1000 in those aged 40 to 49; 1.45 to 1.72 fewer deaths per 1000 in those aged 50 to 59; 1.89 to 2.24 fewer deaths per 1000 in those aged 60 to 69; and 2.68 to 3.17 fewer deaths per 1000 in those aged 70 to 74. For all-cause mortality, RCT data from the prior review reported a non-significant relative reduction in the risk of all-cause mortality of screening mammography for a general population of 1% (RR 0.99, 95% CI 0.98 to 1.00). In this review update, the absolute effects for all-cause mortality over 10 years by age decade were 0.13 fewer deaths per 1000 in those aged 40 to 49; 0.31 fewer deaths per 1000 in those aged 50 to 59; 0.71 fewer deaths per 1000 in those aged 60 to 69; and 1.41 fewer deaths per 1000 in those aged 70 to 74. No observational data were found for all-cause mortality. For overdiagnosis, this review update found the absolute effects for RCT data (range of follow-up between 9 and 15 years) to be 1.95 more invasive and in situ cancers per 1000, or 1 more invasive cancer per 1000, for those aged 40 to 49 and 1.93 more invasive and in situ cancers per 1000, or 1.18 more invasive cancers per 1000, for those aged 50 to 59. A sensitivity analysis removing high risk of bias studies found 1.57 more invasive and in situ cancers, or 0.49 more invasive cancers, per 1000 for those aged 40 to 49 and 3.95 more invasive and in situ cancers per 1000, or 2.81 more invasive cancers per 1000, in those aged 50 to 59. For observational data, one report (follow-up for 13 years) found 0.34 more invasive and in situ cancers per 1000 in those aged 50 to 69. Overall, the GRADE certainty of evidence was assessed as low or very low, suggesting that the evidence is very uncertain about the effect of screening for breast cancer on the outcomes evaluated in this review.</p><p><strong>Conclusions: </strong>This systematic review update did not identify any new trials comparing breast cancer screening to no screening. Although 26 new observational studies were identified, the overall quality of evidence remains generally low or very low. Future research initiatives should prioritize studying screening in higher risk populations such as those from different ages, racial or ethnic groups, with dense breasts or family history.</p><p><strong>Systematic review registration: </strong>Protocol available on the Open Science Framework: https://osf.io/xngsu/.</p>\",\"PeriodicalId\":22162,\"journal\":{\"name\":\"Systematic Reviews\",\"volume\":\"13 1\",\"pages\":\"304\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2024-12-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11656969/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Systematic Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13643-024-02700-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Systematic Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13643-024-02700-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的:本系统综述更新综合了≥40岁女性乳腺癌筛查的益处和危害的最新证据,旨在为加拿大预防保健工作组(CTFPHC)指南更新提供信息。方法:检索Ovid MEDLINE®ALL、Embase Classic + Embase和Cochrane Central Register of Controlled Trials,将检索更新至2023年7月8日。观察性研究的搜索结果仅限于2014年的发表日期,以获取更多相关的研究。筛选由审查小组独立进行,一式两份。为了加快筛选过程,使用机器学习对相关参考进行优先排序。CTFPHC概述的关键健康结果包括乳腺癌和全因死亡率、治疗相关发病率和过度诊断。包括随机对照试验(rct)、非/准rct和观察性研究。数据提取和质量评估由一位审稿人完成,并由另一位审稿人进行验证。使用Cochrane随机对照试验偏倚风险2.0工具和乔安娜·布里格研究所(JBI)非随机和观察性研究清单评估偏倚风险。当认为合适时,研究通过随机效应模型进行汇总。根据GRADE指南评估证据的总体确定性。结果:纳入了3篇报道现有RCT试验数据的新论文和26项观察性研究。本次更新未发现新的rct。没有研究报告了种族、种族、研究人群致密性乳房比例或社会经济地位的结果。对于乳腺癌死亡率,先前综述的随机对照试验数据显示,在普通人群中,乳房x线摄影筛查的乳腺癌死亡率显著降低15% (RR 0.85, 95% CI 0.78 ~ 0.93)。在本次更新的综述中,基于RCT数据的乳腺癌死亡率相对风险降低保持不变,在40至49岁的人群中,10年内按年龄分组的绝对影响为每1000人减少0.27例死亡;50至59岁人群每千人死亡人数减少0.50人;60至69岁人口死亡率每千人减少0.65人;在70至74岁的人群中,每1000人中死亡人数减少0.92人。观察数据显示,相对死亡风险降低幅度为29%至62%。在40至49岁的人群中,10年内乳腺癌死亡率的绝对影响为每1000人减少0.79至0.94例死亡;50岁至59岁人口死亡率每千人减少1.45至1.72人;60岁至69岁人口死亡率每千人减少1.89至2.24人;在70至74岁的人群中,每1000人中死亡人数减少2.68至3.17人。对于全因死亡率,先前综述的RCT数据报告,普通人群筛查乳房x光检查的全因死亡率风险相对降低了1% (RR 0.99, 95% CI 0.98至1.00)。在本次更新的综述中,按年龄划分的10年以上全因死亡率的绝对影响是,40至49岁人群每1000人的死亡人数减少0.13人;50至59岁人口死亡率每千人减少0.31人;60至69岁人群每千人死亡人数减少0.71人;70岁至74岁人群每1000人中死亡人数减少1.41人。未发现全因死亡率的观察性数据。对于过度诊断,本综述更新发现,对于40至49岁的人群,RCT数据(随访范围为9至15年)的绝对影响为每1000例浸润性原位癌增加1.95例,或每1000例浸润性癌症增加1例;对于50至59岁的人群,每1000例浸润性原位癌增加1.93例,或每1000例浸润性癌症增加1.18例。一项去除高风险偏倚研究的敏感性分析发现,在40至49岁的人群中,每1000人中有1.57例浸润性和原位癌增加,或0.49例浸润性癌症增加;在50至59岁的人群中,每1000人中有3.95例浸润性和原位癌增加,或2.81例浸润性癌症增加。在观察数据方面,一份报告(随访13年)发现,在50至69岁的人群中,每1000人中有0.34人患侵袭性和原位癌。总体而言,证据的GRADE确定性评估为低或极低,表明本综述评估的乳腺癌筛查对结果的影响证据非常不确定。结论:本系统综述更新未发现任何比较乳腺癌筛查与未筛查的新试验。虽然确定了26项新的观察性研究,但证据的总体质量仍然普遍较低或非常低。未来的研究计划应该优先研究高风险人群的筛查,比如来自不同年龄、种族或民族、乳房致密或有家族史的人群。系统评价注册:开放科学框架协议:https://osf.io/xngsu/。
Screening for breast cancer: a systematic review update to inform the Canadian Task Force on Preventive Health Care guideline.
Objective: This systematic review update synthesized recent evidence on the benefits and harms of breast cancer screening in women aged ≥ 40 years and aims to inform the Canadian Task Force on Preventive Health Care's (CTFPHC) guideline update.
Methods: We searched Ovid MEDLINE® ALL, Embase Classic + Embase and Cochrane Central Register of Controlled Trials to update our searches to July 8, 2023. Search results for observational studies were limited to publication dates from 2014 to capture more relevant studies. Screening was performed independently and in duplicate by the review team. To expedite the screening process, machine learning was used to prioritize relevant references. Critical health outcomes, as outlined by the CTFPHC, included breast cancer and all-cause mortality, treatment-related morbidity and overdiagnosis. Randomized controlled trials (RCTs), non/quasi RCTs and observational studies were included. Data extraction and quality assessment were performed by one reviewer and verified by another. Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool for RCTs and the Joanna Brigg's Institute (JBI) checklists for non-randomized and observational studies. When deemed appropriate, studies were pooled via random-effects models. The overall certainty of the evidence was assessed following GRADE guidance.
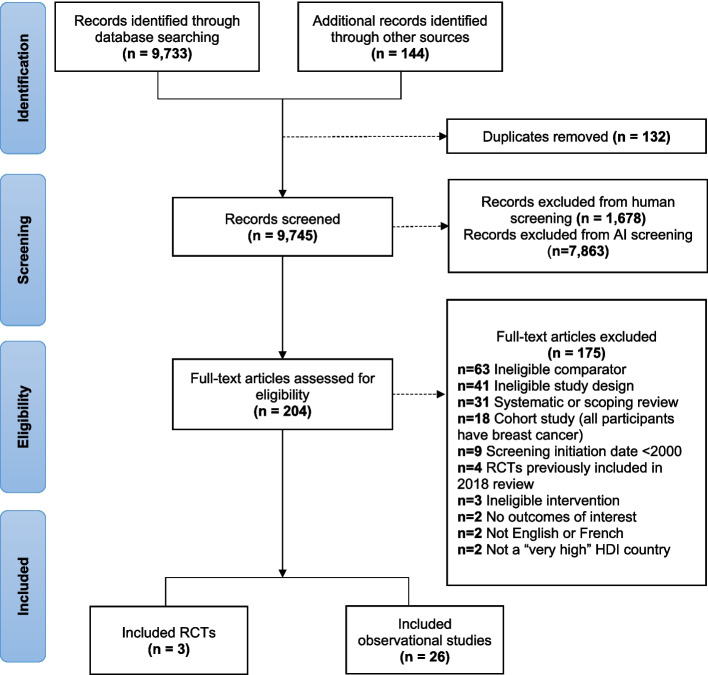
Results: Three new papers reporting on existing RCT trial data and 26 observational studies were included. No new RCTs were identified in this update. No study reported results by ethnicity, race, proportion of study population with dense breasts, or socioeconomic status. For breast cancer mortality, RCT data from the prior review reported a significant relative reduction in the risk of breast cancer mortality with screening mammography for a general population of 15% (RR 0.85 95% CI 0.78 to 0.93). In this review update, the breast cancer mortality relative risk reduction based on RCT data remained the same, and absolute effects by age decade over 10 years were 0.27 fewer deaths per 1000 in those aged 40 to 49; 0.50 fewer deaths per 1000 in those aged 50 to 59; 0.65 fewer deaths per 1000 in those aged 60 to 69; and 0.92 fewer deaths per 1000 in those aged 70 to 74. For observational data, the relative mortality risk reduction ranged from 29 to 62%. Absolute effects from breast cancer mortality over 10 years ranged from 0.79 to 0.94 fewer deaths per 1000 in those aged 40 to 49; 1.45 to 1.72 fewer deaths per 1000 in those aged 50 to 59; 1.89 to 2.24 fewer deaths per 1000 in those aged 60 to 69; and 2.68 to 3.17 fewer deaths per 1000 in those aged 70 to 74. For all-cause mortality, RCT data from the prior review reported a non-significant relative reduction in the risk of all-cause mortality of screening mammography for a general population of 1% (RR 0.99, 95% CI 0.98 to 1.00). In this review update, the absolute effects for all-cause mortality over 10 years by age decade were 0.13 fewer deaths per 1000 in those aged 40 to 49; 0.31 fewer deaths per 1000 in those aged 50 to 59; 0.71 fewer deaths per 1000 in those aged 60 to 69; and 1.41 fewer deaths per 1000 in those aged 70 to 74. No observational data were found for all-cause mortality. For overdiagnosis, this review update found the absolute effects for RCT data (range of follow-up between 9 and 15 years) to be 1.95 more invasive and in situ cancers per 1000, or 1 more invasive cancer per 1000, for those aged 40 to 49 and 1.93 more invasive and in situ cancers per 1000, or 1.18 more invasive cancers per 1000, for those aged 50 to 59. A sensitivity analysis removing high risk of bias studies found 1.57 more invasive and in situ cancers, or 0.49 more invasive cancers, per 1000 for those aged 40 to 49 and 3.95 more invasive and in situ cancers per 1000, or 2.81 more invasive cancers per 1000, in those aged 50 to 59. For observational data, one report (follow-up for 13 years) found 0.34 more invasive and in situ cancers per 1000 in those aged 50 to 69. Overall, the GRADE certainty of evidence was assessed as low or very low, suggesting that the evidence is very uncertain about the effect of screening for breast cancer on the outcomes evaluated in this review.
Conclusions: This systematic review update did not identify any new trials comparing breast cancer screening to no screening. Although 26 new observational studies were identified, the overall quality of evidence remains generally low or very low. Future research initiatives should prioritize studying screening in higher risk populations such as those from different ages, racial or ethnic groups, with dense breasts or family history.
Systematic review registration: Protocol available on the Open Science Framework: https://osf.io/xngsu/.
期刊介绍:
Systematic Reviews encompasses all aspects of the design, conduct and reporting of systematic reviews. The journal publishes high quality systematic review products including systematic review protocols, systematic reviews related to a very broad definition of health, rapid reviews, updates of already completed systematic reviews, and methods research related to the science of systematic reviews, such as decision modelling. At this time Systematic Reviews does not accept reviews of in vitro studies. The journal also aims to ensure that the results of all well-conducted systematic reviews are published, regardless of their outcome.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
